|
Use of Skin-Shock at the Judge Rotenberg Educational Center (JRC) |
IS BEHAVIORAL TREATMENT IMPLEMENTED AT JRC
GENERALIZABLE?
A FOLLOW-UP STUDY OF FORMER JRC STUDENTS
Matthew Israel, Andre Vlok, Joseph Assalone, Rosemary Silva, and Peter Jaberg
Judge Rotenberg Educational Center
Canton, MA USA
This study examines the post-treatment outcomes of 17 former students of the Judge Rotenberg Educational Center (JRC), a residential care facility that employs a highly consistent application of behavioral treatment and educational programming. The students were evaluated approximately 1.5 years (range 0.83 to 3.75 years) after leaving JRC, using both a subjective General Life Adjustment rating (obtained from guardians and former students) and objective counts of certain Quality of Life Indicators. The group of students as a whole showed marked improvement over their status prior to enrolling in JRC on the measures employed.
Introduction
Examining post-treatment outcomes of residential care facilities remains an important aspect in assessing the long-term durability of treatment students receive while in the care of the facility and the generalizability of treatment effects to natural environments. The participants in this study consisted of former students of the Judge Rotenberg Educational Center (JRC). JRC operates day and residential programs for children and adults with behavior problems, including conduct disorders, emotional problems, brain injury or psychosis, autism and developmental disabilities. This study is part of JRC’s on-going efforts to assess the effectiveness of treatment after students have left and to find ways to improve the transition process following residential treatment. The basic approach taken in all of JRC's programs is the use of behavioral psychology and its various technological applications, such as behavioral education, programmed instruction, precision teaching, behavior modification, and behavior therapy and counseling. From JRC's inception, its basic philosophy has always included the following principles: a willingness to accept students with the most difficult behavioral problems and a refusal to reject or expel any student because of the difficulty of his or her presenting behaviors; the use of a highly structured, consistent application of behavioral psychology to both the education and treatment of its students; a minimization of the use of psychotropic medication; and the use of the widest range of effective behavioral education and treatment procedures available[1]. As a result of JRC’s zero-rejection admissions policy, students who attend JRC have included some of the most challenging and difficult students in the nation.
Methods
Participants
The participants consisted of 17 former students of
the Judge Rotenberg Educational Center (JRC). An initial follow-up study was
conducted in May 2003 in which there were 31 participants. A subsequent
follow-up study was conducted in May 2004 consisting of 39 participants. The
follow-up study that was conducted in May of 2005 had 45 participants.
Participants for previous year’s study were selected from a combined pool of the
participants from the previous studies and additional students who had left JRC
within the intervening year. However, in previous studies, no limits had been
established with regard to time since discharge in order to provide the largest
possible pool of potential participants. Although this procedure resulted in a
larger pool of participants, it also resulted in confound related to time since
discharge.
This year, participant follow up data were matched against data from identical time periods prior to admission to JRC. That is, each participant served his or her own control. Thirty-two potential participants were identified as meeting matching criteria and for whom reliable historical data was available.
All of these potential participants had received
comprehensive behavioral treatment during their tenure at JRC. For 23 of these
former students (72%), treatment had consisted of positive-only programming. For
9 of these former students (28%), treatment had consisted of positive
programming supplemented with contingent aversives in the form of a brief skin
shock generated by the Graduated Electronic Decelerator (GED) device[2]. As
reported below, only 17 of these potential subjects were reached for
participation in this current study.
Method
Once potential participants were identified using the selection criteria
described above, their historical information was collected from pre-admission
records for the following areas of general life functioning: psychiatric
hospitalizations, psychotropic medications, legal involvement, day-time
activities and employment status, educational activities, and recreational
activities. Next, the legal guardian of the participant, family member, or the
former student himself or herself was contacted via telephone by a JRC staff
member. During a telephone interview, the respondents were asked a set of
questions from a structured questionnaire, which included identical questions
regarding current dimensions of general life functioning: psychiatric
hospitalizations, psychotropic medications, legal involvement, day-time
activities and employment status, educational activities, and recreational
activities. Thus, indicators of the general life adjustment of participants
before and after treatment were obtained. Guardians were also asked to provide a
general narrative and comments regarding the former students’ performance and to
provide a rating of their general life adjustment based upon a 5-point Likert-type
scale (with 1-very poor, 2-below average/not good, 3-fair, 4-good, and
5-exceptional). These ratings were provided both for present life adjustment and
for life adjustment prior to receiving treatment at JRC.
Results
From an initial total pool of 32 potential participants, 17 (53%) guardians, family members, or former students were successfully contacted As has been the case with the previous JRC follow up studies, the sole reason for inability to contact participants was a lack of current contact information despite extensive measures to maintain contact and obtain current contact information (e.g., repeated phone contacts, searches of information databases such as 411 or Whitepages, etc.).
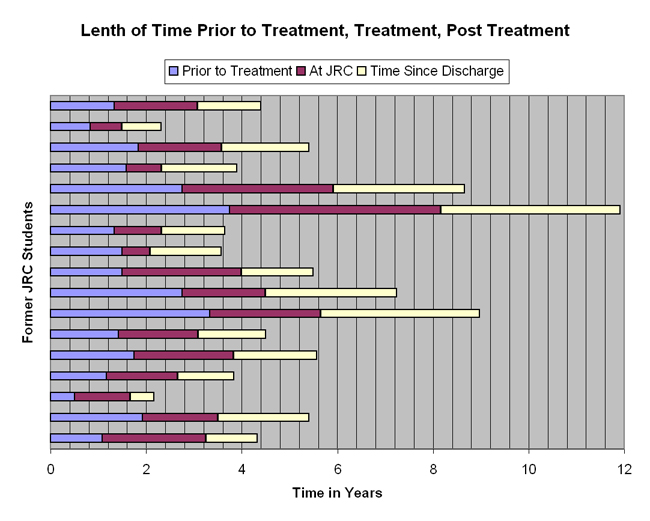
The median age of participants (at the time of this investigation) was 19.8 years with a range of 9.6 to 25.1 years. The median length of stay at JRC was 1.75 years with a range of .58 to 4.42 years. The median time since discharge from JRC was 1.50 years with a range of .5 to 3.75 years. See Figure 1 for frequency distributions of time prior to treatment, length of stay, and time since discharge of each participant.
Figure 1
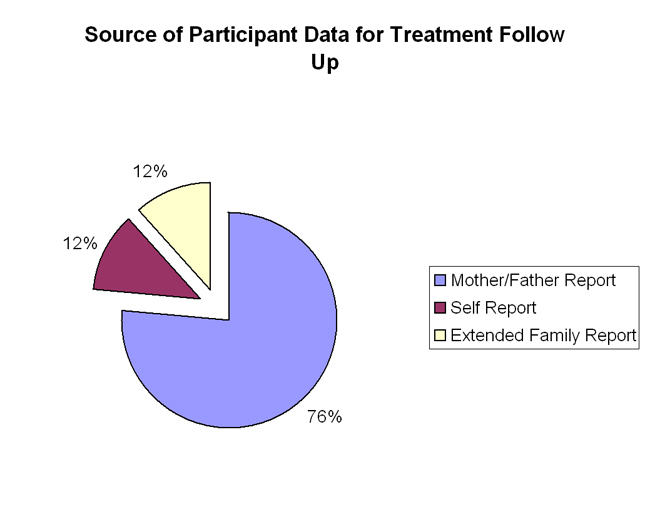
Out of the 17 participants, 11 (65%) received only positive programming. Six participants (35%) received a combination of positive programming with supplemental aversive treatment (see Figure 2). The reporter was a mother or father (either by birth or adoption) in 13 (76%) of the cases, the participant them self in 2 (12%) of the cases, and another extended family member in 2 (12%) of the cases (see Figure 3).
Figure 2
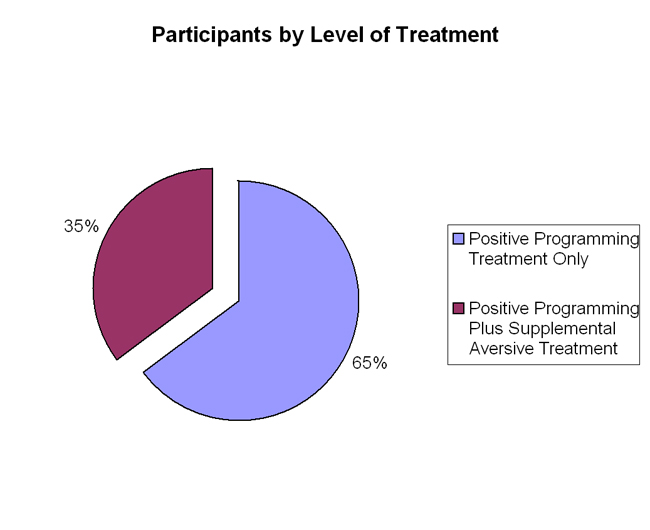
Figure 3
Treatment
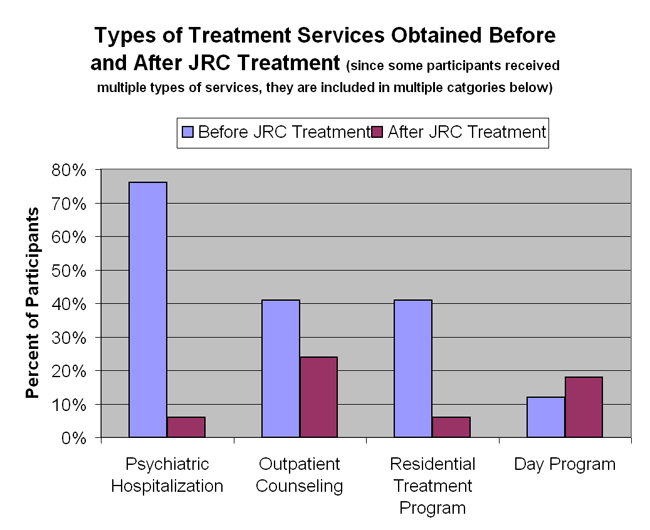
What are the ongoing treatment needs of students after leaving JRC? A comparison was made for each participant’s use of treatment services prior to admission to JRC and following their treatment at JRC. As is shown in Figure 4, the overall number of psychiatric hospitalizations (76% before versus 6% after), use of outpatient counseling (41% before versus 24% after), and use of residential programs (41% before versus 6% after) is much lower following JRC treatment than prior to JRC treatment. The number of individuals using an educational or vocational day program is about the same, but the use of a day program instead of a psychiatric hospitalization or placement away from home in a residential program is a relatively positive outcome. Indeed, some of the individual participants that were requiring the greatest number of psychiatric hospitalizations prior to admission to JRC were the ones that are in day programs upon follow-up.
Figure 4
Psychotropic Medications
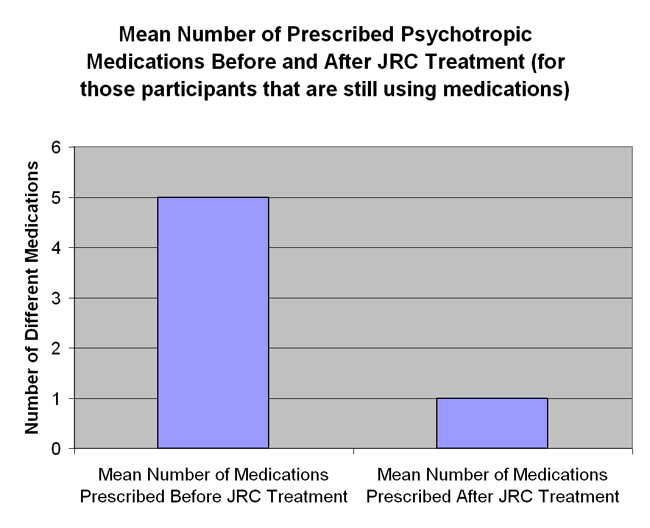
Is there a continuing need for the use of medications following JRC treatment? A comparison was made for each participant’s prescription of psychotropic medications prior to admission to JRC and following their treatment at JRC. As is shown in Figure 5, there is a notable decrease in both the number of participants prescribed psychotropic medications (88% before versus 35% after) and in the mean number of medications prescribed (for those still using prescription medications, see Figure 6) following JRC treatment (5 different medications before versus 1 kind of medication after JRC treatment).
Figure 5
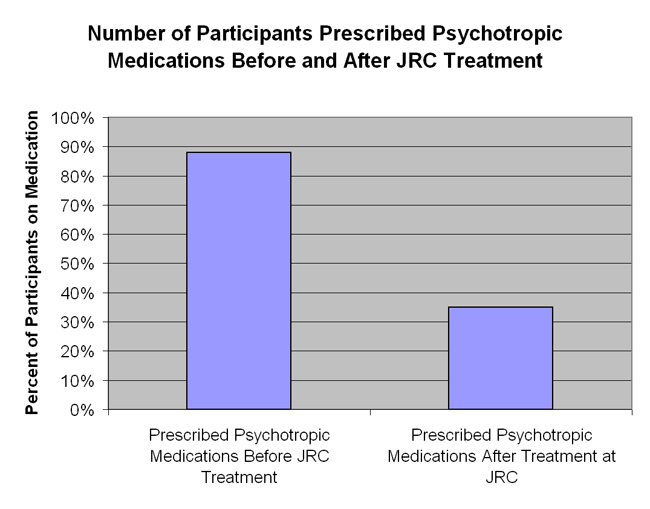
Figure 6
Education
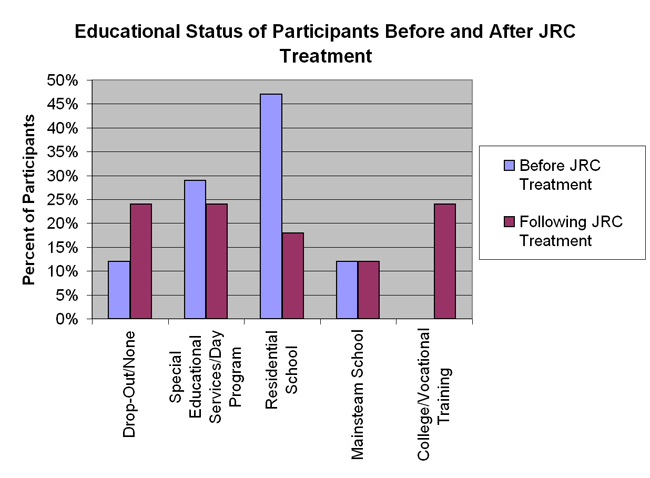
What impact does JRC’s program have on educational functioning? A comparison was made for each participant’s educational needs and programs prior to admission to JRC and following their treatment at JRC. As is shown in Figure 7, the number of students requiring residential educational placement was less following JRC treatment. It should be noted that the number of participants who are classified as receiving no educational services is higher following JRC treatment (12% before versus 24% after). These are mostly participants who have either matured to an age where educational services are no longer mandated by the state or the student has graduated high school (i.e., completed compulsory requirements). This is also reflected by the number of participants (24%) that are currently enrolled in college or vocational school programs after leaving JRC.
Figure 7
Residential Situation
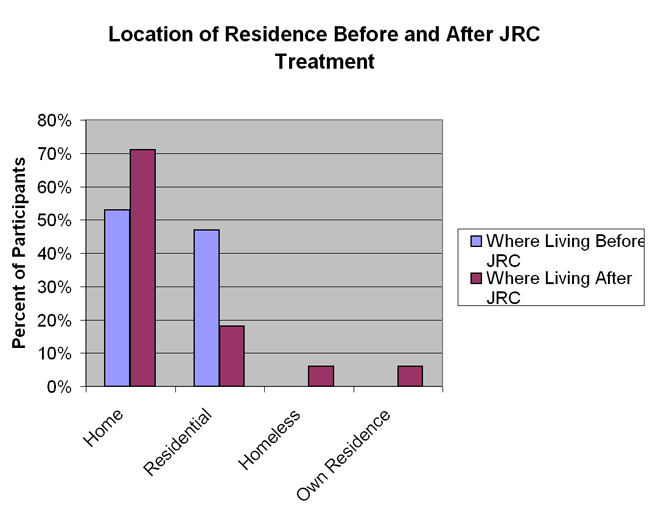
Where are former JRC students living? The comparison of each participant’s living situation prior to admission to JRC and following their treatment at JRC shows (see Figure 8) that there were a fewer number of participants requiring treatment or educational placements away from home (47% before versus 18 % after) and more participants living successfully at home (53% before versus 71% after) following JRC treatment. One participant was homeless and one participant was living independently at the time of follow up.
Figure 8
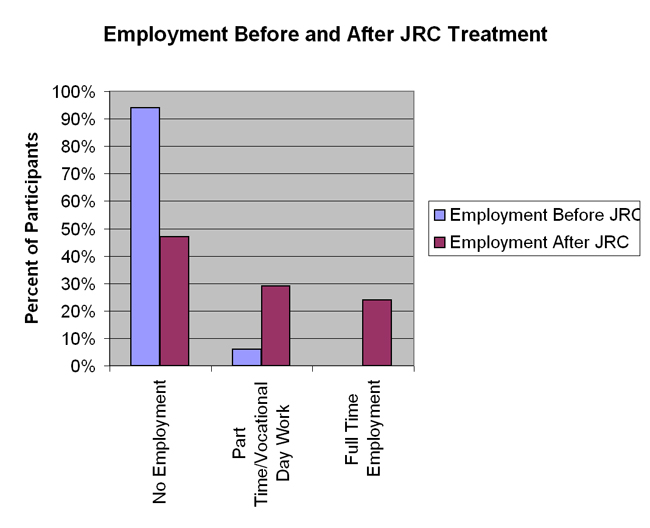
Employment
It is not necessarily reasonable to expect school-age individuals to be working and certainly an increase in employment over a couple of years can be accounted for by maturation. That is, an individual is expected to go to school when they are 16 years old and work when they are 23 years old. That being said, most of JRC’s students enter the program demonstrating behaviors that would prevent them from maintaining gainful employment (in addition to often delayed learning and achievement). At follow up, a quarter of the participants were employed in full time jobs and another quarter of the participants were employed in part time or vocational training positions (see Figure 9). The remaining half of the participants is not currently employed; of these 8 non-employed participants, 6 are currently enrolled in an educational or residential treatment program or are of minor status and thus would not be reasonably expected to be gainfully employed.
Figure 9
Recreation
There is not currently reliable or comparable objective data to report for the quality of recreational activity enjoyed by the participants in this study. Information was collected, but there were no specific criteria or guidelines for how many activities to ask about or other mechanism to further quantify the quality of recreational activity. That being said, the participants reported a wide range of interests and hobbies including: playing basketball, weight lifting, riding roller blades, bicycling, riding motorcycle, taking walks, going to the park/beach, swimming, watching television, playing video games, going out to eat, hanging out with friends, going bowling, reading the newspaper, listening to music, and spending time with their families. As is discussed in the two sections below, the demonstration of inappropriate behaviors interfered with functioning in all aspects of their daily life, including their ability to engage in recreational activities. It appears that the participants are currently engage in a wide range of recreational activities in their personal life.
Relationship Functioning
This area is also typically difficult to quantify. Historical data was collected from social narratives in the participants pre-admission file and is thus limited to what was there in reported. There is likely a bias to report more troublesome aspects of relationship in a typical social history than to focus on positive relationship aspects (although some were noted in the record). For all participants, there was some indication of negative relationship functioning of some type in historical record. In efforts to obtain some consistency and make a meaningful report of relationship functioning, each participant’s data was checked for whether they currently have friend/peer/dating relationships where they had poor peer relationships or “no friends” specifically noted in their historical records. Of the participants for whom this specific level of data is available (8 of 17 participants, 47%), all indicated improvement in relationship functioning with specific statements indicating positive friendship or dating relationships. There is one participant that reports no apparent improvement in relationship functioning and two participants for whom no data is available.
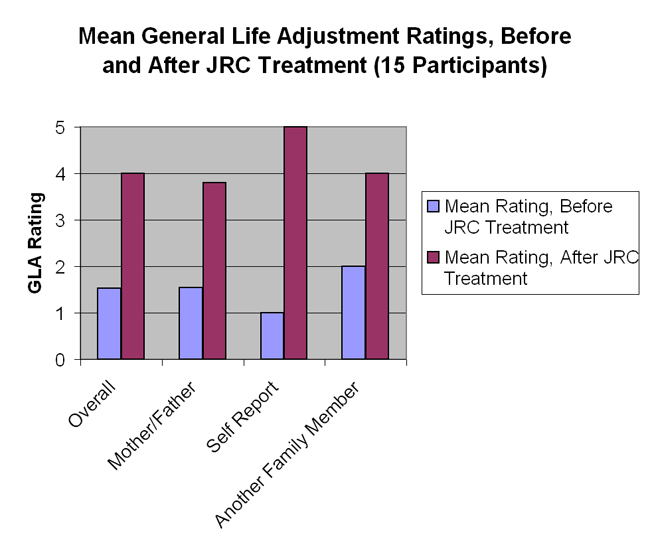
General Life Adjustment Rating
See Figure 10 for comparisons of mean before and after JRC general life adjustment (GLA) ratings (by mother/father, self, or another family member). These subjective ratings are vulnerable to a number of report biases, but do reflect a genuine perception of the respondents that the participant’s overall level of functioning has continued at an improved level since discharge from JRC. Ratings are available for 15 of the 17 participants (88%).
Figure 10
Discussion
The results of this investigation indicate that former students of JRC demonstrated marked improvement in their life adjustment and quality of life following treatment. These findings are consistent with follow-up studies from three previous years.
The marked improvement, as indicated by the data for these participants, serves as evidence that not only have indicators for quality of life improved since starting treatment at JRC, but that this improved functioning has continued for as long as 3.5 years after the participant was discharged from JRC. After leaving JRC, students from this study transitioned back home, to another less restrictive residential program, or to a day educational/vocational program. Some of these students started full or part time jobs and some pursued further (post-secondary) education. For others, to be able to safely return home and have relatively normal family and peer relationship is an indicator of treatment success.
Limitations of the current study included the small sample size. This was partly the result of more stringent selection criteria and efforts to control of length of time for history and time since discharge. As with previous follow-up studies conducted at JRC, there was relatively high attrition due to the inability to locate current contact information for a significant number (47%) of the initially selected participants. The ability to successfully contact the guardians of former students remains a significant aspect in assessing the long-term treatment effects of residential programs. Maintaining more frequent on-going contact with guardians of former students, as well as the former students themselves, may increase the ability to track the follow-up progress of more students in the future.
In conclusion, although there were several factors that limited the generalizability and significance of the findings, the results indicate that former students of the Judge Rotenberg Educational Center showed substantial overall improvement as measured by the indicators of quality of life as used in this study.
Suggested areas of improvement that might be considered to enhance future follow-up studies of residential care include the following additions: (1) a standardized symptom or behavioral checklist administered at pre-admission, at discharge, and at specified periods post-discharge; (2) a control group consisting of students accepted into the facility, but not attending; (3) an examination of the relationship of pre-admission variables (e.g., number of previous placements, intellectual functioning, and prior
adjudication) to post-treatment outcomes; (4) an examination of the relationship of other variables (such as time since discharge, length of stay, reason for discharge, etc.) to post-treatment outcomes; and (5) further examination of ratings in terms of statistical significance as quantifiable.
Possibly the most important aspect of collecting and examining post-treatment data for residential care is to identify better ways to improve the transitional process and quality of life for former students. To this end, JRC continues to implement a Follow-Up Program, which includes the components listed below: (1) Periodic telephone calls to the former student, guardians, and day activity agency (e.g., school, day treatment program, Job Corps, etc.) to ascertain status and make suggestions for helpful intervention, (2) Occasional visits to the student by JRC staff, (3) On-going email communication with student by JRC teachers and administrators (4) Behavior contracts for good performance established (and rewards provided) by JRC, present day activity agency, or guardians, (5) Continued self-management assistance from JRC to promote good performance in post-JRC environments, (6) Offer of training to personnel involved with student in post-treatment setting, (7) Invitation to student to contribute information on progress to an online database including: (a) behavior frequency counts collected by student, guardian, or others, and (b) periodic prose reports or comments on student’s progress and status, (8) Special online discussion board for former students and staff to promote continued communication and support, and (9) Instituting follow-up support six months prior to discharge to facilitate transition.
Taking these additional steps may assist in maximizing the general life adjustment and quality of life for former students by allowing for minimally restrictive continued treatment efforts, communication, and support through the gradual reduction of components of successful residential care.
[1] Additional information is available from JRC’s website at www.judgerc.org.
[2] The GED is a remote-controlled skin-shock device which delivers brief, mild electrical stimulation to the surface of the skin. The reader is referred to www.effectivetreatment.org/remote.html for a detailed paper regarding the development and characteristics of the GED. Additionally, a case study documenting the effectiveness of positive programming supplemented with contingent aversives in the form of the GED can be found at www.effectivetreatment.org/treat.html.