|
Use of Skin-Shock at the Judge Rotenberg Educational Center (JRC) |
SEVEN CASE STUDIES OF INDIVIDUALS EXPELLED FROM POSITIVE-ONLY PROGRAMS
Matthew L. Israel, Nathan A. Blenkush, Robert E. von Heyn, and Christine C. Sands
Judge Rotenberg Educational Center
Canton, MA USA
Abstract
In the debate over
aversives a little-known but significant fact is often overlooked: programs that
restrict themselves to positive-only treatment procedures sometimes expel
individuals with severe behaviors when their behaviors become too difficult to
handle. We review seven such cases of individuals with severe behavior problems
who were expelled from state-of-the-art, positive-only programs and describe
what happened to them when they were enrolled in a program that was able to
supplement its positive-only procedures with contingent skin-shock when
necessary.
Key words: severe
behavior, skin-shock, aversives, positive behavior support
Seven Case Studies
of Individuals Expelled from Positive-Only Programs
Many problem behaviors of
special needs individuals can be satisfactorily treated with “positive-only”
behavioral treatment procedures. By “positive-only” we mean behavioral
procedures that do not include physical aversives. Support for the effectiveness
of positive-only procedures in treating many individuals can be found in a
comprehensive review by Carr et al. (1999). They showed that in 50% of the
studies that qualified for their review, the behaviors were successfully treated
(using a standard of achieving a 90% reduction from baseline) with positive-only
procedures, and that this figure rose to 60% when the cases reviewed were
limited to those in which a functional analysis was performed.
Despite the fact that
40-50% of the cases in the Carr et al. (1999) report were not effectively
treated, proponents of positive-only programming continue to assert that
all severe problem behaviors can be
managed successfully with positive-only procedures. For example, the TASH
presents the following information on their website, “Positive
strategies for changing behavior work equally rapidly, work with behaviors that
are equally severe, and ar
Foxx (2005) made two
important points in response to thes
The present paper presents
a third point relating to th
This paper presents seven
brief case histories of individuals who were expelled by
behaviorally-sophisticated, positive-only programs when their behaviors became
too difficult to manage. All seven were subsequently admitted to the Judge
Rotenberg Educational Center (JRC), a program that is able to supplement
positive-only procedures with a contingent skin-shock aversive when required.
For a description of the treatment procedures employed at JRC, see
The positive-only programs
that expelled the seven individuals discussed below, ar
All information and
quotations provided below have been taken from referral documents provided to
JRC as part of the normal enrollment process for each of the individuals
involved. In each case, the parents of these individuals have granted permission
to JRC to use their child’s information in this paper1. The
individuals whose data are displayed will be referred to as Students 1, 2, 3,
etc. and the schools as School A, B, C, etc.
Student 1
Between th
School A tried many
“positive-only” treatment approaches without success. They gave Student 1
rewards of small snacks, breaks, and preferred activities throughout the day
contingent on appropriate behaviors or on the completion of certain tasks. They
taught Student 1 functional communication responses, in which he used language
to request being alone, to get teacher attention, or to escape demands. They
tried using restraint as a positive reinforcer for desired behaviors. They
provided Student 1 with periods of no demands and periods of high-rate demands.
At one point Student 1 received 1-1 staffing during all waking hours. School A
made use of internationally-recognized experts in the behavioral treatment of
sever
In March, 2005, School A
expelled Student 1. His Discharge Summary explained the reason as follows: “At
this point, behavior-control medication and treatment approaches based on
positive reinforcement have been generally unsuccessful in producing
long-lasting decreases in Student 1’s behavior. This suggests that Student 1 may
requir
In March 2005, at age 15,
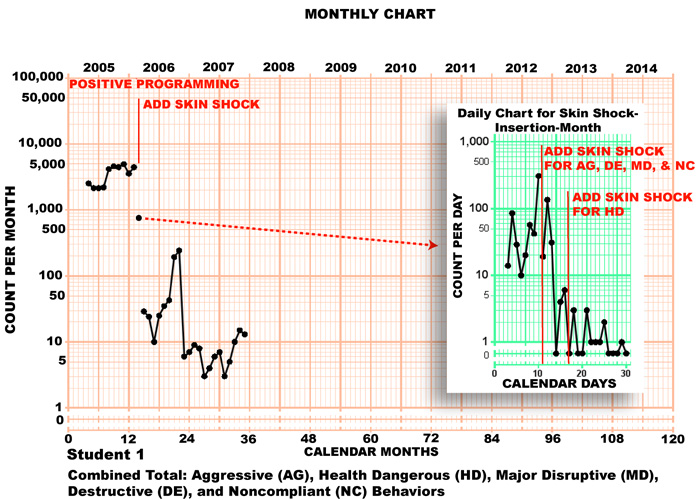
Student 1 was admitted to JRC. Figure 1 is a chart showing combined monthly
totals of Student 1’s aggressive, health dangerous, major disruptive,
destructive, and noncompliant behaviors.
Figure 1.
The effect of contingent skin-shock on th
The chart is the same2
as the monthly version of the Standard Celeration Chart (Pennypacker,
Guiterrez & Lindsley, 2003) except that it displays only 5 of the usual 6
cycles. The chart has a multiply/divide scale on the vertical axis. A relative
change, such as a doubling, tripling or halving, occupies a constant up-down
distanc
The data series displayed
on the left side of Figure 1 is divided into three parts: (1) a data series for
the 10 months of baseline (labeled “Positive Programming”); (2) a single data
point for the month during which the skin-shock was inserted in the student’s
program (the “skin shock insertion month”); and (3) a data series for 21 months
of skin-shock treatment. The data point for the skin-shock insertion month is
not connected to either the baseline or treatment series because it contains
some days from the baseline phas
To show the data for each
of the days of the skin-shock insertion month there is a daily chart that is
inset on the right side of the chart3. This chart is basically the
sam
Figure 1, as well as the
other behavior charts included in this paper, shows the number of behaviors that
the individual in question engaged in, and not the number of skin-shock
applications, which was always less. One reason is that sometimes the individual
displayed many instances of certain behaviors within a single episode. In such
cases each separate behavior occurrence was tallied and recorded, but only one
skin-shock application was given to consequate the entire episode. Another is
that on some occasions, due to equipment failure or other reasons, an
alternative consequence (a verbal “No”) was substituted for the skin-shock.
During Student 1’s first 10
months at JRC, psychotropic medication was tapered and discontinued, and
positive-only programming was used exclusively. Figure 1 shows, however, that
JRC’s positive-only programming was not successful by itself in decreasing
Student 1’s problem behaviors. Over the course of his first 10 months at JRC, he
displayed a mean of 3,532 aggressive, health dangerous, major disruptive,
destructive, and noncompliant behaviors per month and the behaviors wer
After these first 10
months, during which JRC’s positive programming proved unsuccessful, Student 1’s
parents gave their approval to JRC to supplement his positive programming by
arranging a
single skin-shock
consequence for each instance of his problem behaviors. For more information on
JRC’s positive-only programming procedures and its use of supplementary
skin-shock delivered by the Graduated Electronic Decelerator (GED) device4,
see
The data for the first
month of treatment are displayed in the inset daily chart on the right side of
Figure 1. Notice that CSS treatment of health dangerous behaviors (labeled “HD”
in the inset) began one week after CSS treatment was started for the other four
categories of behavior—aggressive (AG), destructive (DE), disruptive (DI), and
noncompliant (NC). The relatively high rates seen during the first few days of
CSS treatment reflect the continued high rate of Student 1’s health dangerous
behaviors, which were not yet being treated with CSS.
Once skin-shock was added
to Student 1’s program for all of his major problem behaviors, the behaviors
showed an abrupt drop in monthly frequency, changing from 4,459 during the last
full month of baseline data to 29 during the first full month of CSS treatment—a
decrease in which the frequency divided by a factor of 154. In calculating this
drop, immediately after CSS insertion, for Student 1 (and for the other students
covered in this paper) we ignored data from the skin-shock insertion month,
because it was composed of data from both the baselin
In the 21 months since skin
shock was started with Student 1, the rate of his major problem behaviors has
remained at a manageably low level. Although his problem behaviors are not at
zero, his most recently monthly frequency was only 13 as compared with 4,459 in
the final baseline month.
As a result of this
dramatic decrease in Student 1’s problem behaviors, by April, 2006, he was able
to participate in weekly academic and recreational field trips to places such as
restaurants, art centers, the zoo and bowling alleys. He was able to complete
his bathroom routine independently and had learned to brush his teeth with only
verbal prompts. As of this writing, Student 1 works independently on his
computer academics and completes most of his household chores without the need
for prompts. His family now enjoys successful visits with him at JRC and takes
him into the community on those occasions.
Student 2
In 1999, at age 13 Student
2 enrolled in a day school operated by School B, another
well-regarded special needs program that uses positive-only behavioral treatment
procedures. At that time she engaged in head-banging to the point of causing
pain, redness, bruising and tissue damage. She did this by either hitting her
head against an object or by punching her head or face with her fist. Sh
School B treated these behaviors using the following positive-only procedures: they tried to block all of her self-injurious behaviors; they prompted her to put her hands down if necessary; they stopped interacting with her until she remained calm for ten seconds; they encouraged her to use her “words” instead of exhibiting her problem behaviors; they granted any request during times she was not exhibiting her behaviors; they gave her a functional communication book and they also used manual restraint in the form of certain “protective holds.” On the school bus they kept a row of empty seats as well as an aisle between Student 2 and the nearest other person. In addition, the psychotropic medications Buspar, Prednisone, and Risperidone were tried without positive effects. Student 2’s last IEP from School B shows that her self-injurious behaviors, even after 5 years of positive-only treatment, were occurring approximately 23 times per day.
In April 2004, School B
expelled Student 2. Shortly thereafter, at age 17 she was admitted to JRC.
Figure 2 is a monthly chart showing Student 2’s aggressive, health dangerous and
noncompliant behaviors, all combined into one monthly total.
Figure 2.
The effect of contingent skin-shock on th
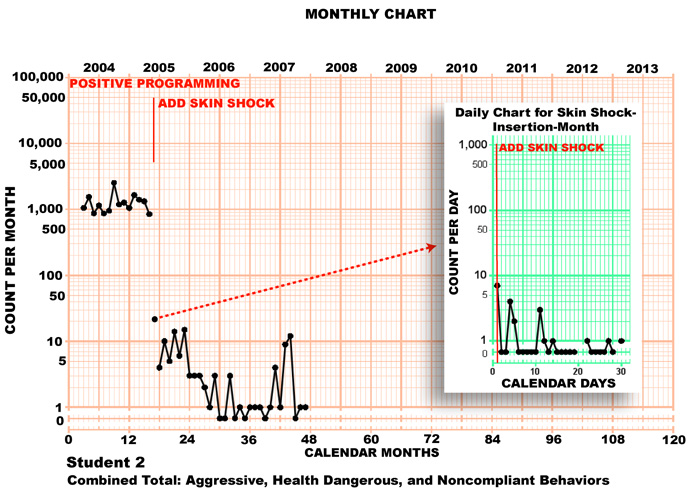
During her first fourteen
months at JRC, Student 2 was treated with positive-only programming. This was
not effective in decreasing her major problem behaviors which, after fourteen
months, were still occurring at unacceptably high levels (mean of 1,994 per
month during the last three baseline months).
In May 2005, JRC added a
skin-shock intervention to Student 2’s program to treat her aggressive, health
dangerous behaviors, and noncompliant behaviors. Figure 2 shows that once the
skin-shock consequence was added, her aggression, self-abuse, and noncompliance
decreased abruptly. After skin-shock insertion, and ignoring the data from the
skin-shock insertion month itself, Student 2’s problem behaviors dropped from
848 per month (last full baseline month) to 4 per month (first full treatment
month)—i.e., divided by a factor of 212. Those behaviors then decelerated
further over the next 2 ½ years, except for a sudden frequency increase (“jump
up”) in July 2007 and a sudden frequency decrease (“jump down”) in September
2007, and reached 0 or 1 during each of the last 3 months shown on the chart.
Student 2 now engages in
academics for extended periods and is able to move from on
Student 3
Between th
When Student 3 exhibited
these problematic behaviors, the primary techniques that School A employed were
“physical intervention,” placing him in “exclusionary time out” (seclusion) and
restricting him from “community and vocational environments for varying amounts
of time depending on the topography of the behavior.” Positive interventions
utilized whil
On
Figure 3.
The effect of th
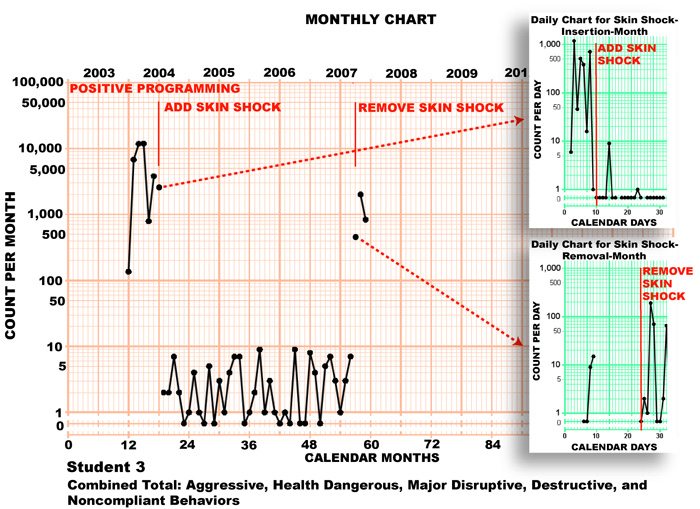
These behaviors included
aggressive, health dangerous, destructive, major disruptive behaviors and
noncompliant behaviors. During Student 3’s first six months at JRC, he received
positive-only programming including, for example, various behavior contracts
targeting th
Student 3’s problematic
behaviors showed little improvement during his first five months at JRC. On
month 6 he was still exhibiting 3,828 dangerous behaviors per month (a mean of
128 per day)—an unacceptably high level. There were some days, prior to the
introduction of skin-shock, on which Student 3 would exhibit over 2,000
dangerous behaviors including aggression and sexually inappropriate behaviors.
In June of 2004 (daily data
for this month is shown in the top inset graph) skin-shock was added as a
consequence for Student 3’s major problem behaviors. As soon as the skin-shock
treatment was added to his program, Student 3 showed sudden and dramatic
improvement. The frequency of his problem behaviors showed an immediate
frequency decrease from 3,828 per month on the last full baseline month (and
again ignoring the data for the skin-shock insertion month) to 2 per month on
first full treatment month—an improvement by a factor of 1,914. After that, and
for the next three years, Student 3’s major problem behaviors maintained at a
very low level, between 0 and 9 per month.
From the summer of 2004
through March 2007, Student 3 was able to work consistently each day on his
academic skills in a classroom with his peers. He no longer hurt himself or
others. He lived in an apartment with his peers that had minimal staffing, was
learning vocational skills and went on several successful home visits.
In March, 2007 Student 3
ran away from JRC and when he returned his mother withdrew her permission (at
Student 3’s request) for the skin-shock treatment. Once this treatment was
removed, Student 3’s behaviors regressed to the same levels that he had shown at
the end of his baseline period of “positive-only” treatment. The return of
Student 3’s problem behaviors as soon as skin-shock was removed shows how
critical the skin-shock was for his improved behavior and suggests that for him
it was functioning at that tim
Currently Student 3 is
doing poorly and his mother is now considering granting permission onc
Student 4
Student 4
enrolled in School C at th
School C did a
careful functional analysis of Student 4’s behavior problems and attempted to
treat him with a wide variety of positive-only procedures which included the
following: use of a picture schedule both in school and in the residence; use of
a set of “first….then” sequence cards with him so that he could anticipate
reinforcement; use of a timer so that he could recognize the beginning and end
of activities; a sensory diet; instruction that was short, direct and brief; use
of a penny board; use of a “break card” so that he could request a break at any
time; use of communication book; and functional communication training.
In addition,
Student 4 was given medications such as Haldol, Dexedrine, Orap, Thorazine,
Risperdal, Depakote, Clonidine, Cogentin, Benydryl, Zoloft, and Luvox. Thorazine
was also prescribed as a PRN, and if his behaviors failed to respond to the
Thorazin
School C
eventually decided that it was unable to meet Student 4’s needs and sought to
refer him to some other program that might be better able to manage his
behaviors. Every appropriate placement in his home state rejected Student 4
after reading his history. His information was then sent to 18 schools from
A crisis period
for Student 4 developed just prior to the point when he was discharged from
School C. During this crisis, various additional interventions were tried,
including retraining the staff that worked with him, providing 1:1 staffing at
all times, psychiatric consultation, consultation with a well-known expert in
autism, classroom changes, hospital outpatient psychiatric services, and PRN
medications.
Eventually
Student 4 was referred to JRC, which accepted him.
In
December of 2004, at age 19, Student 4 was discharged from School C and
transferred directly to JRC. Upon arrival at JRC, Student 4 went into a coma due
to an overdose of psychotropic medication that was given prior to and during his
transportation to JRC. He was diagnosed with Neuroleptic Malignant Syndrom
Figure 4 is a
monthly chart for Student 4 in which each data point represents the total of all
of Student 4’s most dangerous behaviors during that month.
Figure 4.
The effect of contingent skin-shock on th
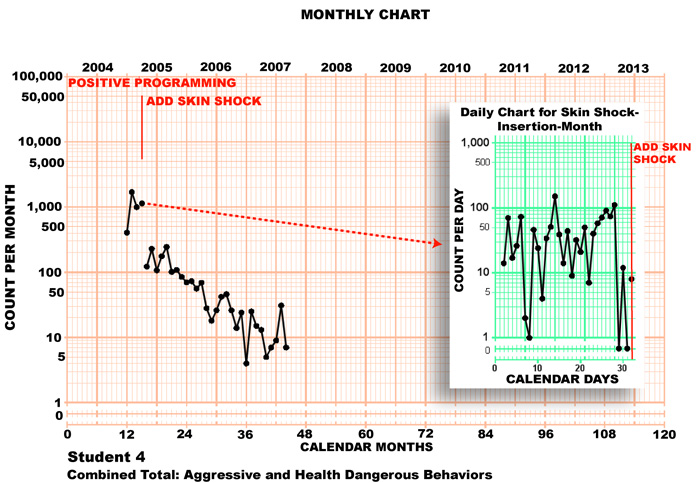
The chart shows
that during his first 3 months at JRC, during which he received positive-only
treatment, Student 4 displayed a mean of 1,038 aggressiv
Student 4 is
now completely off all psychotropic medications and works daily on a computer
doing his academic work. Student 4 has also made significant progress socially
and with his daily living skills. He is able to participate in academic and
recreational field trips, attends all school activities and goes out into the
community with his parents when they visit, without any JRC staff accompanying
him.
Student 5
Student 5
attended School A as a residential student between th
School A tried a variety of
positive-only behavioral strategies. These included “positive reinforcement
contracts,” as well as “antecedent-based” types of interventions (manipulation
of stimuli and setting events). At one point, after receiving expert
consultation from a behavioral consultant, School A implemented new reward
procedures as well as punishments. Contingent upon good behavior, C.M was
allowed to a) select who would work with him on an hourly basis, b) choose from
any preferred item or activity and c) request breaks and conversations at any
time. In addition, surprise rewards were delivered on a variable-time schedule.
Following certain maladaptive behaviors, Student 5’s behaviors were consequated
by providing him with complete (but non-preferred) meals and denying him any
form of social attention until he exhibited 8 consecutive hours of appropriate
behavior. This social isolation procedure was not effective. Whil
Student 5’s referral
summary reports that although School A’s treatment procedures often showed
promis
In an IEP amendment dated
Figure 5.
The effect of th
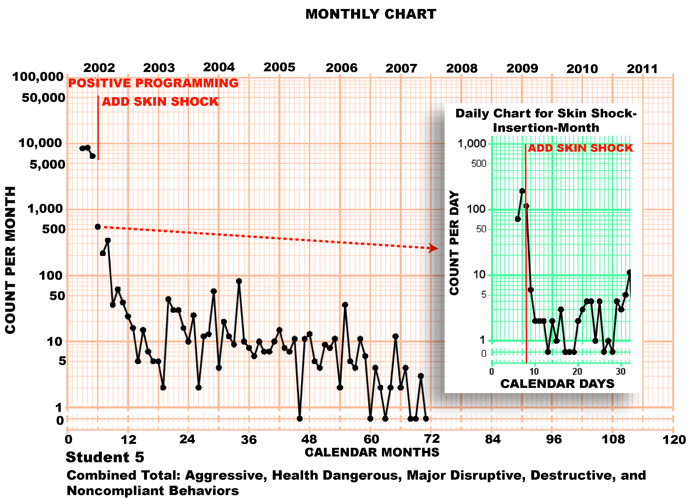
During Student 5’s first
four months at JRC, psychotropic medications were tapered and discontinued, and
positive-only programming was applied. Although this programming succeeded in
dropping his major problem behaviors from a frequency of 8,626 per month to
6,502 per month, this was still an unacceptably high level.
In June of 2002 JRC added a
skin-shock intervention to his program, with the usual prior parental consent,
individual court authorization and other safeguards. Figure 5 shows that this
addition to Student 5’s program was associated with an immediate frequency jump
down. Onc
Student 5 now rarely
requires physical restraint and consistently masters academic lessons in
reading, math, phonics and spelling. He lives with another student in an
attractively decorated room which he does not damage. He enjoys field trips
(educational and recreational) and no longer has difficulties with transitions.
Student 5 continues to learn new and appropriate social behaviors that hav
Student 6
In September 1997, Student 6, at age 14, displayed such sever
School D’s
interventions to treat Student 6 included mechanical restraint for almost the
entire day, and immobilization at night. He was even prevented from moving while
in bed in order to help him sleep better. Despit
In March 2000,
Student 6 was discharged from School D and sent back to the children’s hospital
from which he had come. The hospital continued the use of the restraint that had
been developed at School D and later, due to his continued aggressiv
At age 17, in
October 2000, Student 6 was admitted to JRC. At that point he was in mechanical
restraint and still receiving Droperidol and Cogentin. Whenever Droperidol, an
anesthetic, was administered to him, Student 6 fell asleep. He was weaned very
quickly from the psychotropic medications because they appeared to have no
therapeutic value in view of the fact that he still exhibited intens
Figure 6 shows
the combined monthly totals for Student 6’s aggressiv
Figure 6.
The effect of contingent skin-shock on th
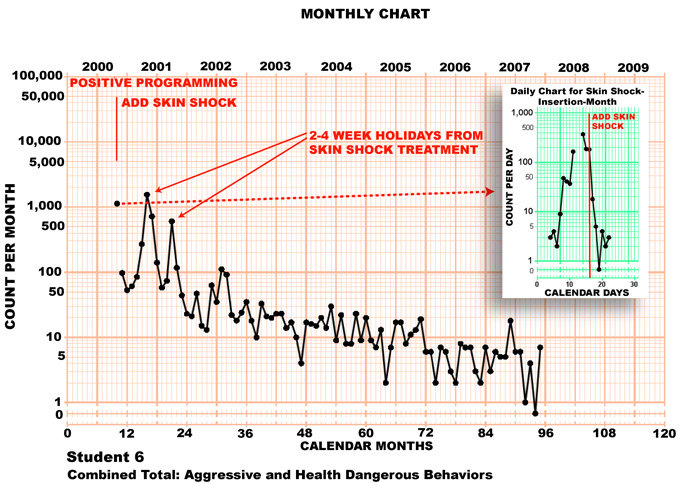
Within one week
of th
Student 6 is now
flourishing academically and socially.
He is free of all restraint and medication. H
Student 7
Student 7 was enrolled in special education programs starting at th
Student 7 was
then admitted to the same School A that is referred to above. At that point he
was engaging in 70-80 aggressiv
Student 7 then
spent 7 years at School F. School F’s interventions included the use of group
dynamics, art, music, academics and th
School F was
unable to treat Student 7 successfully and at age 12 he was removed and enrolled
in School G. Whil
One of the
principal interventions used at School G involved escorting him to a secluded
area subsequent to an aggressive or health dangerous episod
Figure 7.
The effect of contingent skin-shock on th
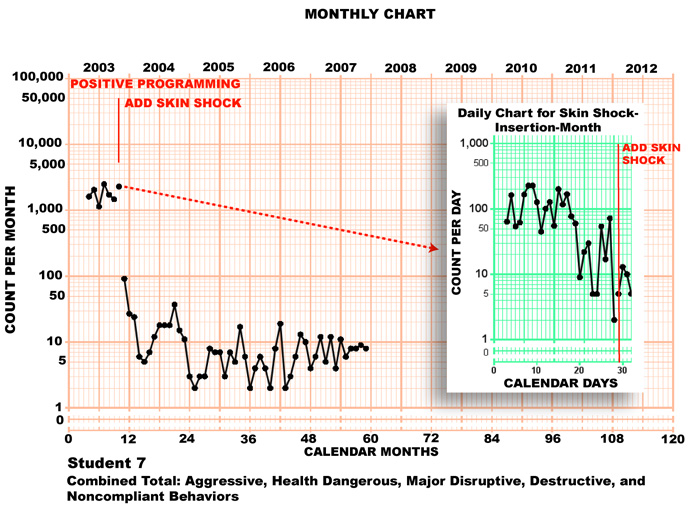
When Student 7
was admitted to JRC he was treated with positive-only programming for over six
months. During this period there was no deceleration in his problem behaviors
and he was engaging in a mean of 1,753 dangerous and disruptive behaviors per
month. After these six months of positive-only programming, contingent
skin-shock was added to Student 7’s treatment. Student 7’s health dangerous,
aggressive, destructive, major disruptiv
In addition to
these behavioral improvements, Student 7 advanced academically and socially. As
of October, 2003 when skin-shock was inserted into his program, Student 7 was
able to participate in community outings and weekly field trips to places such
as museums, amusement center, and restaurants and was able to go on frequent
home visits with his family.
Discussion
All seven
individuals presented in this paper were expelled from highly regarded
behavioral programs that used state-of-the-art positive-only programming. All
seven eventually required that their positive-only programs be supplemented with
an effectiv
These reports
also suggest that th
References
Association for
Positive Behavior Support. (2007, February)
PBS Standards of Practice: Individual
Level. Retrieved
Carr, E. G., Horner, R. H.,
Turnbull, A. P., Marquis, J. G., Magito McLaughlin, D., McAtee, M. L., Smith, C.
E.,
Foxx, R. M.
(2005). Severe Aggression and
Self-Destructive Behavior: The Myth of the Nonaversive Treatment of Severe
Behavior. In J. W. Jacobson, R. M. Foxx, & J. A. Mulick (Eds.),
Controversial Therapies for Developmental
Disabilities (pp. 295-310).
Pennypacker, H. S.,
Guiterrez, A., & Lindsley, O. R. (2003).
Handbook of the standard behavior chart.
TASH. (n.d.).
Positive Behavior Supports.
Retrieved
van Oorsouw, W. M. W. J.,
Author Contact Information
Matthew L. Israel
email:
m.israel@judgerc.org
Nathan A. Blenkush
email:
n.blenkush@judgerc.org
Robert E. von Heyn
email:
r.vonheyn@judgerc.org
Christine C. Sands
St Augustine, FL 32084
(904) 540 – 9107
email:
drsands@bellsouth.net
Author’s Note
Matthew L.
Christine Sands is now Director of Behavioral Services at
Adams Acres.
We thank
Correspondence concerning this paper should be sent to:
Matthew L.
Footnotes
1
Copies of the
documents containing the quotations contained in this document, as well as
related information, ar
2
As is true of the monthly Standard Celeration
Chart, on this chart a data series that doubles every six months draws a 34
degre
3
The reader may wonder why the first data point
on this inset daily chart is not placed on the first vertical line. On this
daily chart the heavy vertical lines represents Sundays, and the thin vertical
lines represent the weekdays. Each data point is plotted on the day of the week
appropriate to the date on which the student displayed that total number of
problem behaviors.
4
For an analysis of
the side effects of JRC’s skin shock treatment, see