|
Use of Skin-Shock at the Judge Rotenberg Educational Center (JRC) |
The Successful Use of Contingent Skin Shock Following Years of
Positive-Only
Programming: Two Case Studies Using a Multiple Baseline Across Individuals and
Behaviors with Long Term Follow-Up
Robert E. von Heyn, Matthew L. Israel and Maryellen Kelley
Judge Rotenberg Center, Canton MA USA
The Judge Rotenberg Educational Center operates day and residential programs for children and adults with behavior problems, including conduct disorders, emotional problems, brain injury or psychosis, autism and developmental disabilities. The basic approach taken in all of JRC's programs is the use of behavioral psychology and its various technological applications, such as behavioral education, programmed instruction, precision teaching, behavior modification, behavior therapy and behavioral counseling. From JRC's inception, its basic philosophy has always included the following principles: a willingness to accept students with the most difficult behavioral problems and a refusal to reject or expel any student because of the difficulty of his or her presenting behaviors; the use of a highly structured, consistent application of behavioral psychology to both the education and treatment of its students; a minimization of the use of psychotropic medication; and the use of the most effective behavioral education and treatment procedures available.
Introduction
Critics of the use of aversive procedures typically state
that positive only programming is effective to reduce severe maladaptive
behaviors in all individuals. For most individuals admitted to JRC,
positive-only treatments were successful. However for some individuals more
intrusive treatments were necessary to successfully decelerate their dangerous
behaviors. The two individuals presented below received positive-only
programming, primarily using multiple DRO contracts, for 2 to 3 years before the
treatment was supplemented with contingent skin shock. Prior to the use of skin
shock the inappropriate behaviors had decelerated significantly but were still
maintained at an unacceptably high rate. In addition, frequent use of emergency
physical and mechanical restraint were necessary. Data are presented in a
multiple baseline design. Data for one individual depicts a rapid deceleration
to zero rates while other showed a gradual deceleration over a period of years.
In both cases the contingent skin shock procedure was gradually eliminated and
both individuals maintained their gains.
Method
Participants
The families of the two individuals presented were not able to maintain them safely at home. In addition, they were discharged from previous placements due to the programs inability to control the severity of their aggressive and self-injurious behaviors. Both were adolescents, with a diagnosis of mental retardation, with little or no verbal skills. Neither were able to receive an education as their behaviors significantly interfered with learning. Teacher could not be within arms length due to their aggression and it nearly impossible to present and materials without having them destroyed.
CL
· Admitted to JRC June 1995 at the age of 13
· Diagnoses of severe mental retardation, seizure disorder and cerebral palsy
· Psychotropic medications included Mellaril and Elavil
· Behavioral interventions included in wheelchair restraint, one-to-one staffing, positive behavioral programming and a specialized day program.
GR
Procedure
Both participants were initially treated with highly structured behavior plans that used a variety of Differential Reinforcement of Other Behaviors (DRO) contracts. Contract lengths varied between 5 minutes and 24 hours, depending on the frequency of the targeted behaviors. Reinforcers were individualized for each participant and were based on their preferences. A token economy was also in place for each participant. Tokens were awarded for passing contracts, completing academics or exhibiting other defined pro-social behaviors. Tokens could be spent in a variety of ways to purchase preferred items or activities. A response cost system was also in place whereby tokens were deducted when targeted behaviors occurred. When participants exhibited aggressive or self-injurious behaviors, emergency physical or mechanical restraints were employed. Chemical restraint was never used. For more information on JRC’s programs visit www.judgerc.org.
For these participants, the positive only approach did
produce clinically significant improvement in their targeted behaviors but their
rates maintained at an unacceptable rate. These behaviors interfered with their
entire educational and habilitative programming and posed a significant risk of
injury. After 6 months JRC began, with Court permission, using a contingent food
program and protective gear, in an attempt to further decelerate their
behaviors. These additional treatments did not clinically reduce the maladaptive
behavior to an acceptable level and therefore, at 23 months (GR) and 34 months
(CL), JRC petitioned the Probate Court in Massachusetts for permission to use
the Graduated Electronic Decelerator (GED) to treat their challenging behaviors.
The GED was an FDA registered medical device that administers a 2-second skin
shock when remotely activated by a therapist. The proposed treatment plan
presented to the Court and written by a doctoral level psychologist or clinician. The
treatment plan operationally defined the behavior topographies JRC requested for
treatment with the GED. When GED treatment began, the individual’s daily
recording sheet described those topographies for which the clinician
prescribed GED treatment. To insure reliable treatment, two therapists confirmed
the existence of the targeted behavior on the individual’s daily recording sheet
before the GED consequence was administered. Twenty-four hour a day videotaping
and live monitoring also insured treatment consistency. For more information on
the GED see
www.effectivetreatment.org.
Results and Discussion
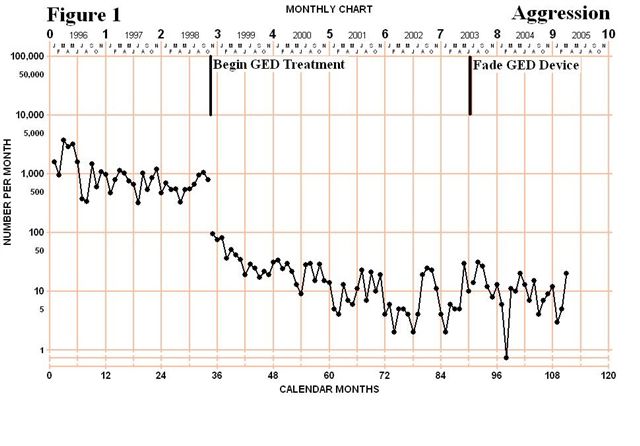
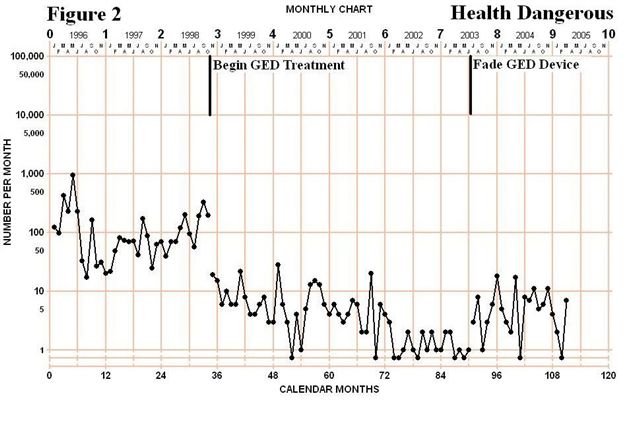
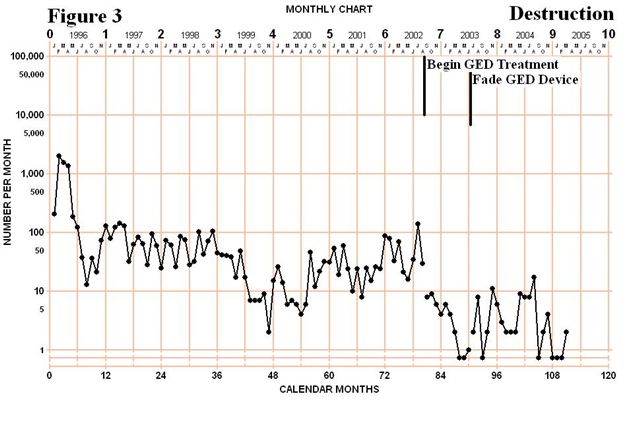
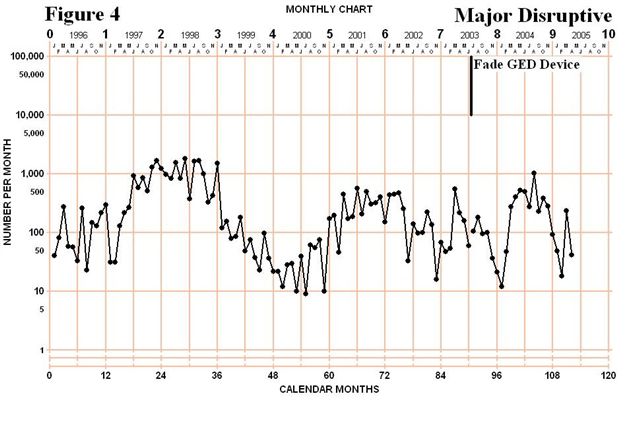
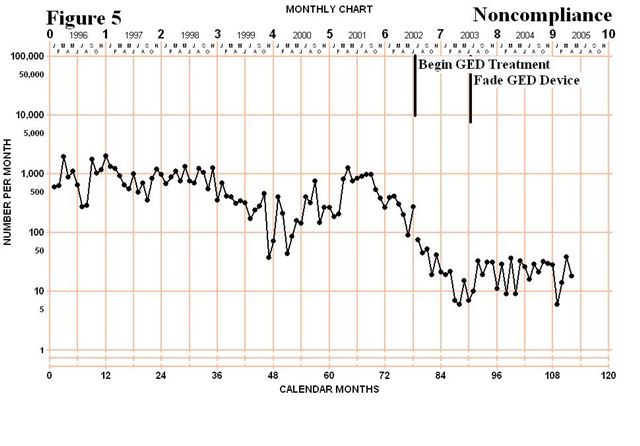
Figures 1 and 2 depict the total monthly frequency of CL’s aggressive (AGG) and health dangerous behaviors (HDB). The phase lines indicate the beginning of treat with the GED for specific behaviors. GED treatment began for her aggressive and health dangerous behaviors in November 1998 and led to an immediate 10-fold decrease in the rate of these behaviors. Over the next 4.5 years the rate of these behaviors continued to decelerate in both frequency and intensity. The onset of GED for AGG and HDB was also followed by a deceleration of her major disruptive behaviors (MDIS) shown in Figure 4. More than 3 years later GED treatment began for her NCMP behaviors in July 2002 which led to a further deceleration of these behaviors but did not seem to affect any of the other categories of behaviors that were not being treated with the GED. Finally, treatment began for her destructive behaviors in September 2002 and, again, produced an immediate and sustained improvement but no collateral affect on her other categories not treated with the GED. Major disruptive behaviors such as yelling and screaming, which were never treated with the GED, have remained highly variable but not systematically affected by the successful treatment of her other behaviors. As indicated on the charts, the GED contingencies was used for an extensive period of time, but was faded out almost completely eliminated from her treatment program.
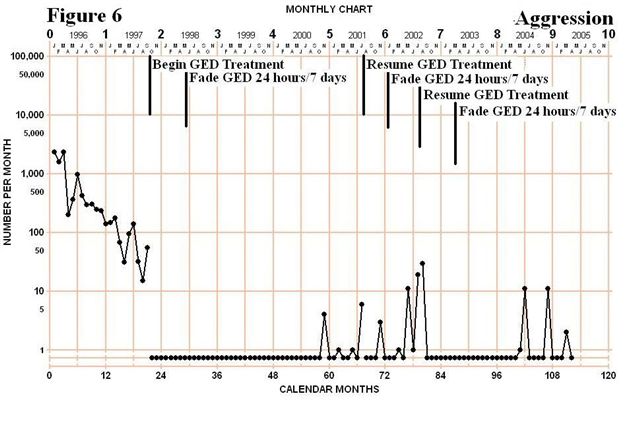
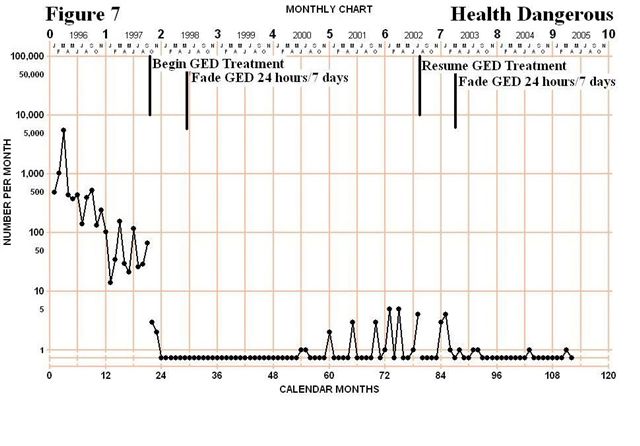
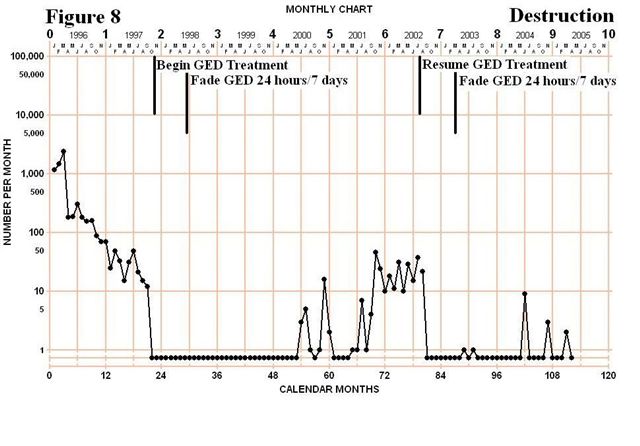
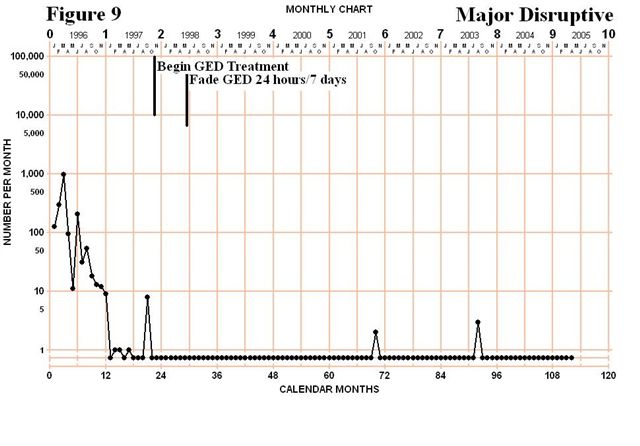
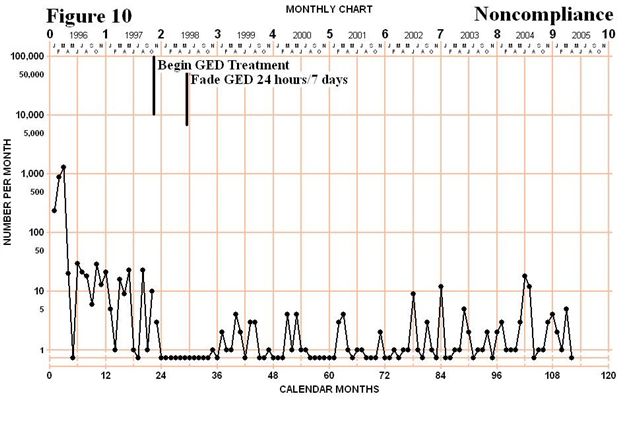
Figures 6 to 10 depict the total monthly frequency of GR’s AGG, HDB, DES, MDIS and NCMP. For GR, GED treatment began in September 1997 for AGG and HDB and in October1997 for DES, MDIS and NCMP. What is clear across charts is that the introduction of the GED led to a rapid deceleration to zero when it was made contingent on that behavior category. Two other interesting results also occurred with GR. First, when treatment began for AGG and HDB his DES behavior also decelerated to zero even though the contingency did not change for that behavior category. Secondly, GR’s NCMP behavior was unaffected by the introduction of the GED to other categories but immediately went to zero when GED was made contingent on NCMP behaviors. Figures 6, 7 and 8 show that the GED was faded from his program in less than a year and the positive programming maintained his behavior for a few years. However, once in August 2001 and again in August 2002 a short reinstatement of the contingency was necessary due to some intense aggressive behaviors and frequent destruction. In both cases within a few months the GED was removed from his program and has remained off for the past 28 months.
Conclusion