|
Use of Skin-Shock at the Judge Rotenberg Educational
Center (JRC) |
| |
print this page
USE OF ELECTRICAL STIMULATION IN BEHAVIORAL TREATMENT AT THE
JUDGE ROTENBERG EDUCATIONAL CENTER (JRC www.judgerc.org)
(Note: When viewing the links (Exhibits) you
must use your browser's back button to return to this page.)
Matthew L. Israel, Ph.D.
Judge Rotenberg Educational Center
- Overview of Judge Rotenberg Educational Center (JRC) Program
- Residential educational/treatment program for individuals with severe
behavior problems
- Facilities
- Students are transported each school day to and from JRC’s
administration/school building in Canton, MA, USA. See
Exhibit 1.
- Students live in apartments and homes in Canton and surrounding communities.
See Exhibit 2.
Student Population: currently (as of July 10, 2000) JRC serves 110
individuals
- 67% are under the age of 22. 33% are over 22.
- 49% are individuals with developmental disabilities. 51% are higher
functioning individuals with emotional/behavior problems.
Basic Policies:
- JRC maintains a near zero rejection/expulsion policy,
assuming that parents/guardians grant permission for all needed treatment
procedures. As a result of this policy:
- JRC treats individuals with case-hardened behaviors:
- The average student with developmental disabilities at JRC has been
ejected by 5 programs and rejected by 6 potential placements
- JRC serves what is probably the highest concentration of severely
autistic-like students in the country.
JRC tries to minimize use of psychotropic medication.
- Reasons:
- We wish to avoid their sometimes-damaging side effects. Sometimes these
effects are irreversible and not known until years after the medication is
first introduced;
- Psychotropic drugs are often of only limited usefulness in treating
specific behavior problems;
- Controlled experimental data supporting their use is sometimes
inadequate;
- Some psychotropic medications are more intrusive than behavioral
procedures;
- Psychotropic medications sometimes succeed only at the cost of putting
the individual into a kind of stupor.
- Psychotropic medication is used, however:
- when behavioral procedures are insufficiently effective;
- when a combination of behavior modification and psychotropic medication
is the most effective, least intrusive treatment; or
- when psychotropic medication is well-recognized as a treatment of choice
for a specific psychiatric disorder
- Over the past 10 years, 72 students have received supplementary skin shock
aversives as part of their treatment program at JRC. Only one of these 72
has also used psychotropic medication
JRC seeks to minimize the use of restraint.
Only 1 out of the 72 students who have received supplementary skin shock
aversives as part of their treatment program has needed to be in continuous
partial restraint
JRC operates a highly structured and consistent 24-hour behavior
modification program.
Program
JRC is certified as a school and offer an educational program that features
behavioral approaches to education:
- Individualized, self-paced instruction is used in which each student works
at his/her own speed and must master each material before advancing to the
next.
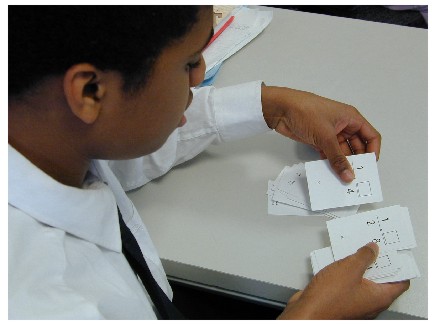
- Precision teaching in the teaching of skills and in the measurement of
progress.. See Exhibit
3, for
example, which shows a student using flash cards and measuring own
rates correct and incorrect.
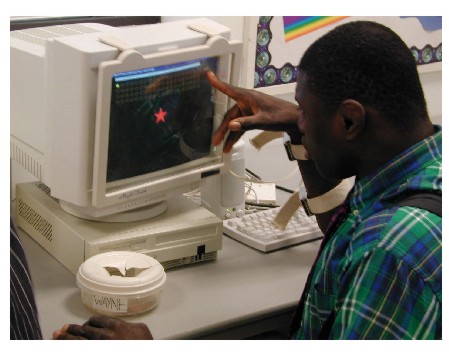
- Computers are used as teaching machines.
- We have designed our own software to teach basic skills. See Exhibit
4, which shows a student using our own software
that teaches pointing, matching and reading letters and numerals.
- For higher functioning students we have designed special software to
teach spelling, vocabulary and math facts, as may be seen in the
accompanying photograph. See
Exhibit 5.
Student computers in the classrooms are networked, with access to the
internet. See Exhibit
6.
For higher functioning students there is a computer in each bedroom at the
residences. See Exhibit
7.
For higher functioning students, The school provides a ratio of one
computer for each student.
Behavior modification is used to motivate student performance, through a
comprehensive point system. Points are earned through both academics and
behaviors and spend on various rewards described below.
The primary emphasis in treatment is on the use of positive programming
procedures. JRC has developed a varied and comprehensive positive
reward program that is extremely powerful and that is the dominating feature of
the program. The following are aspects of JRC’s positive programming:
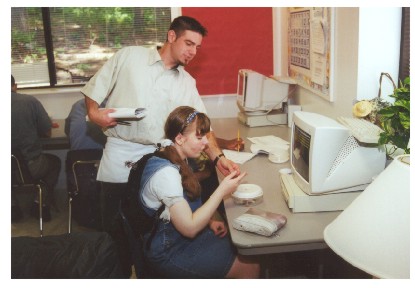
- Intermittent, Momentary Verbal Rewards.
- Staff members are trained and supervised to catch the student,
throughout the day, at times when he/she is behaving appropriately and to
administer a casual reward that consists of some attention, and some money
or points.
- We try to give 5 or 10 of these each hour to each student, if possible.
See the accompanying photo, which shows a staff member giving one of these
casual rewards, consisting of attention, a smile, physical contact and a
penny. See Exhibit
8.
Contract rewards for not displaying problematic behaviors. JRC sets up
a wide variety of "behavioral contracts" in which if the student can
display certain behavior during a certain period of time, he/she earns a
reward. The various types of contracts that are standard with each student
are:
- Less-than-a-day
- One day
- Overnight
- Transportation
- Multi-day (often weekly)
- Special (made for task completion, behaviors on field trips, etc.
A wide variety of reward opportunities are provided. Some examples of
these reward opportunities are these:
- Classroom reward store
. Many of the classrooms of the
developmentally disabled students have a couch setup with TV and music
system, games, etc., within the classroom. Students can earn a chance to
take a break and relax in this area by meeting certain classroom goals or
contracts. See Exhibit
9 which shows a typical classroom reward store.
- Reward box.
This is a box of desired items that students can rent
or buy to take home as part of the reward system. See Exhibit
10.
Contract store. This is an in-school store
with many items that are attractive to our students. The students can pick
out an item and then make a behavioral contract to earn the item. See Exhibit
11.
Big (School-Wide) Reward Store. See Exhibit
12 and Exhibit
13 which show an arcade-like room
that contains video games, a pool table, vending machines, etc.
Reward afternoon. See
Exhibit 14. Once a week there is a special
barbecue with fun activities which the students can also earn through their
behaviors.
Dances See Exhibit
15.
Recreation equipment in each bedroom, including
a TV, stereo, CD player, and Sony playstation. There is also a computer,
some with internet access. The internet is probably the single biggest
reward item for the higher functioning students. See Exhibit 16.
Self management projects Each student chooses
an outer and an inner behavior of his/her own to work on and reports and
discusses his project with a group of other students who are also working on
their own self-management projects. See Exhibit 17.
Behavioral counseling. We have a staff of
Ph.D.-level behavioral psychologists and clinicians who provide counseling from a
behavioral perspective that is closely coordinated with the ongoing behavior
modification program. See Exhibit
18.
Use of optional, supplemental aversives.
If positive programming alone proves
insufficiently effective, we add the use of supplementary aversives. Currently
the only aversive we employ is a remote-controlled skin shock device.
- 1971-1989—Use non-shock aversives.
- The principal types of aversives employed are:
- Water squirt (plant spray bottle);
- Vapor spray (compressed air mixed with water)
- Pinch, slap, and muscle squeeze
- Aromatic ammonia
- White noise/visual screen helmet
- Mechanical restraint
- Combinations of procedures
- Results are:
- Improvement, but nowhere near improvement with GED
- Many students still in partial restraint, including helmets, for
substantial parts of day
- Continuous struggles to restrain students--sometimes 4 restraint
boards in a classroom, occupying entire floor area
- Injuries to staff, students and property
In 1989-90, we began our use of remote-controlled skin-shock as an aversive.
Safeguards were set up which are:
- Approval by parents guardians
- Substituted Judgement Legal Authorization
- Human Rights Committee
- Peer Review Committee
- Medical and psychiatric sign-off re no contraindications
- Daily nursing Review
- Tight control and management of direct care staff
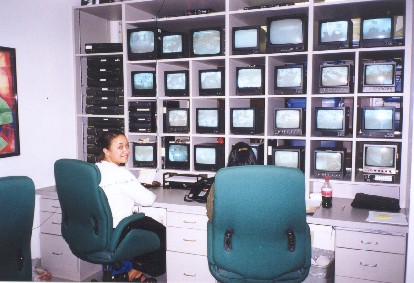
- Program Monitoring
- Live video monitoring of activities in all areas of school during school
hours. See Exhibit
19.
- Multiplex videotaping of activities in all areas of residences during
evening and overnights and subsequent spot-checks by a videotape
review staff.
- Monitoring personnel during day, evening and overnight who make
unannounced visits to classrooms and residences.
Extensive charting of all behaviors
- A Daily Behavior Recording Sheet follows the student throughout the day
and evening. See Exhibit
20.
- The frequency data derived from this Recording Sheet are plotted on four
types of Standard Celeration Charts:
- Daily Frequency. See Exhibit
21
,
- Weekly Frequency. See Exhibit
22,
- Monthly Frequency. See Exhibit
23.
- Yearly Frequency.
Films Showing Students Before and After Treatment
(To request a copy of this
film, please e-mail Karen LaChance at k.lachance@judgerc.org.
Please include your name, address, and phone number and put "Before and
After Film" in the subject line.)
- JRC’s 11 years of experience in the use of skin-shock
- JRC’s Use of Skin-Shock
- Major methods employed
- Wide variety of behaviors treated
- Health Dangerous (Includes Self-Abuse)
- Aggression
- Property destruction
- Noncompliance
- Inappropriate Urination/Defecation
- Major disruptive Behaviors
- Use on earliest possible antecedents
- Use on "shaped-down versions" of behavior
- Simultaneous use on all behavior targets at same time
- Preventive use in form of behavior rehearsal lessons
- Use of holidays to help stimulation to recover its effect after apparent
adaptation
- Occasional use in negative reinforcement paradigm
- Consistent application by direct care staff, 24 hrs/day, in all settings
including shower
- Occasional use to punish refusals in the form of intentional wrong answers
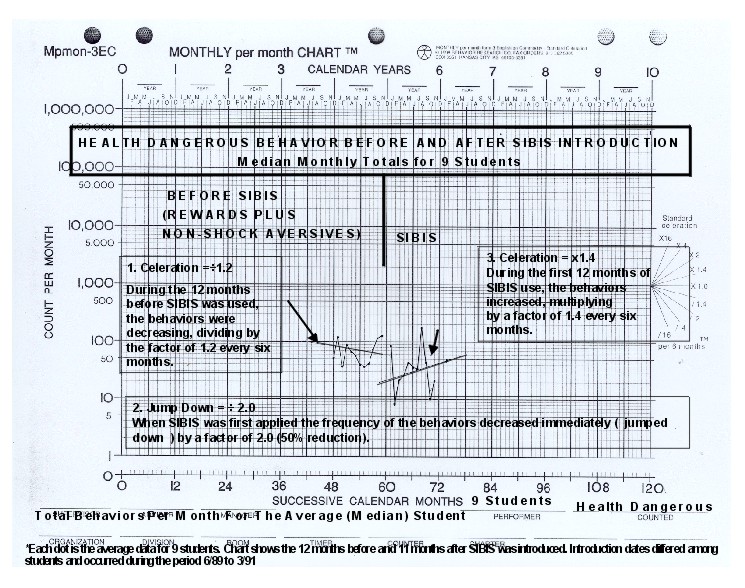
1989-90 Use of SIBIS (Self-Injurious Behavior Inhibiting System) device.
Our experience with SIBIS is summarized in
Exhibit
24.
- Exhibit 25
is a chart comparing the effectiveness of nonshock aversives
versus the use of SIBIS for 9 students (12 months before the introduction of
SIBIS and 11 months after)
- Chart shows little effect.
- Totally ineffective for some
- Only temporarily effective (2-6 months) for most
- Counter-therapeutic (accelerating) for a few
- Device unsatisfactory
- Insufficient intensity
- Did not give a true indication the shock has been administered—only that
signal from remote control unit was received
- Not sufficiently rugged (too fragile) for 24-hour use.
- Short battery life
1990: Design and use of the GED (Graduated Electronic Decelerator) Device
and GED4
Exhibit 26 is a table comparing the features of SIBIS
with the GED and the GED4 (a stronger version of the GED)
The important thing to note is the amount of current produced by each:
- SIBIS’ current of 2ma (rms)
- GED’s current is 15ma (rms);
- GED4: 45.0 ma rms)
Intensity is adjustable, but in practice we have always used it as its
highest level
Duration: 2 seconds, fixed period
1-5 electrode pairs used on same student
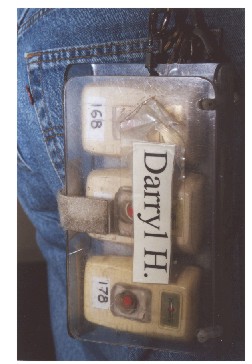
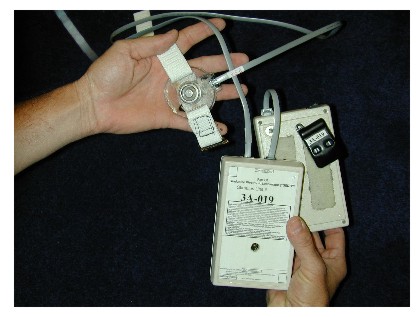
The GED Device and its components
Remote transmitter. See Exhibit
27 and Exhibit
28.
- Note that photo shows three separate transmitters. Each is for a different
electrode site.
- We use from 1-5 electrodes in different sites on each student.
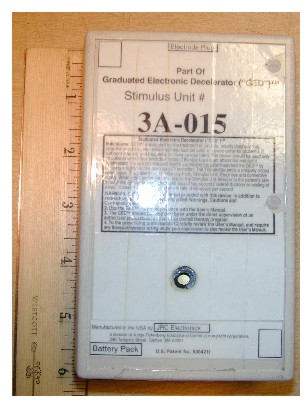
Stimulator. See Exhibit
29.
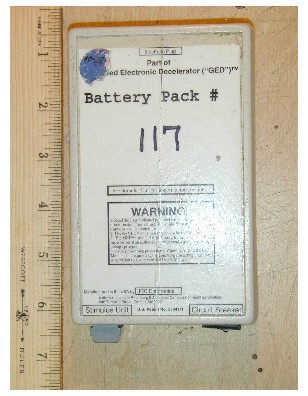
Battery. See Exhibit
30.
Battery pak holder. See Exhibit
31.
Electrode separated from the stimulator chassis by a wire shown in Exhibit
32 allows the electrode
to be placed on almost any area of the body. See Exhibit
33.
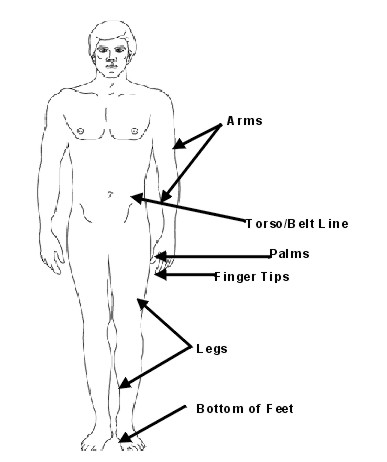
Electrodes
- Concentric. See Exhibit
34.
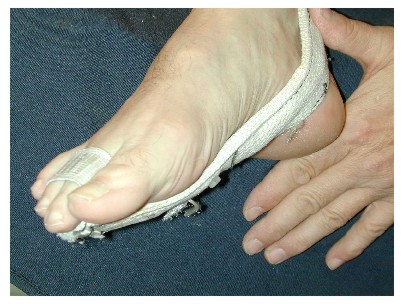
Spread (See Exhibit
35) electrode:
2 electrode buttons separated from each other by up 6 inches
- This enhances the effectiveness of the stimulation
- Spread is normally used on arms or legs, but can also be used on hands
or feet.
- Spread: finger to palm
(Exhibit
36)
Spread: Finger to finger (Exhibit
37)
Spread: Bottom of foot (Exhibit
38)
Device gives an auditory signal that indicates actual current flow, not just
that the unit has received signal from the remote controller. (Cf. SIBIS,
where indicator signal signals only that signal from transmitter has been
received by the receiver.)
Chart showing comparison between SIBIS or Nonshock aversives vs. GED, for 36
students (Exhibit
39)
shows GED to be very effective.
- For 36 students, we examined their 12 months immediately before GED was
introduced (they were on either SIBIS or non-shock aversives) and their 11
months after.
- Note that this is not a calendar time chart. Students were started on the
GED on different calendar dates. But the data for the first, second, third,
etc. months before and after has been grouped together for purposes of this
summary chart.
- Immediate "jump-down" in frequency by a factor of 5.
- Where the behavior had been accelerating before GED, it showed a deceleration
after the GED was introduced (after the immediate jumpdown).
Exhibit 40
summarizes our experience with
GED and GED4, 1989-date: Experience with Skin Shock
- Effectiveness
GED has proven effective on 60 of 66 students for whom we have complete
data.
For the 6 for whom GED was not effective, or lost its effect, we designed a
stronger version called GED4. This was effective in 5 of the 6 students.
Success rate for GED/GED4= 98%
Exhibit 41 also shows the amount of experience JRC has had with skin
shock
- GED and GED4: 316 years
- SIBIS, GED and GED4: 354 years
- Number of applications: over half a million
- We believe this to be the single most extensive experience in the use of
skin-shock of any agency.
Exhibit 42 shows the distribution of
students arranged by years of experience with the GED.
- Median length of use is 4 years, range 1-10
The median frequency of application
for each student currently (this has been true for about 6-7 years)
- Across all students, medial is 3.5 applications per week (less than 1
two-second application per day)
- For 37% of users, median is 0/week.
The following are individual charts
each of which illustrates one interesting point of our experience.
-
Exhibit 43
shows
Gabe’s chart. It
illustrates an "immediate "cure.".
- Exhibit
44
is the chart for Jessica. It
illustrates the effectiveness of verbal mediation.
-
Exhibit 45
is the chart for Heather. It
illustrates the usefulness of a holiday from GED use, in order to promote
recovery of effectiveness of stimulation after apparent adaptation.)
-
Exhibit 46
is the chart
for Epifanio. It shows the superiority of the spread electrode over the
concentric electrode. It also illustrates the greater effectiveness of the
spread electrode when as applied to the fingers over the spread electrode as
applied to the arms or legs.
-
Exhibit 47
is a chart for
self-abuse for Greg, who was one of the students shown in the before-and-after
film. We combined the use of behavioral rehearsal lessons with the use of skin
shock when the behavior actually occurred. During the behavioral rehearsal
lessons, Greg was physically prompted to engage in the initial phases of a
self-injurious act and then given a skin shock. This was done 4 times per day.
As never engaged in a full example of a self-abusive act in the eight years he
has been with us. The only instances that were consequated naturally (as
opposed to being consequated in the course of the lessons) were threats to
engage in the behavior or the very beginning phases of the behavior.
-
Exhibit 48
is a chart for
Lourdy’s aggression. In his case punishment of the complete acts of
aggression were effective in causing a jump-down in the frequency, but the
behavior did not decelerate at that, remaining an an unacceptable frequency of
about 20 per month. However, when we began to punish out-of-seat, which was
the beginning phase of the behavior, combined with negatively reinforcing the
behavior of returning to his seat (by ceasing the use of intermittent
skin-shock), the behavior decelerated toa near-zero level.
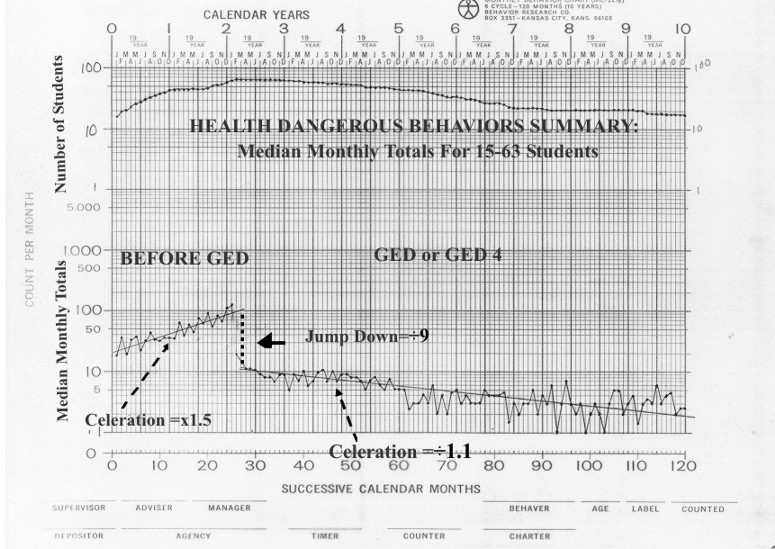
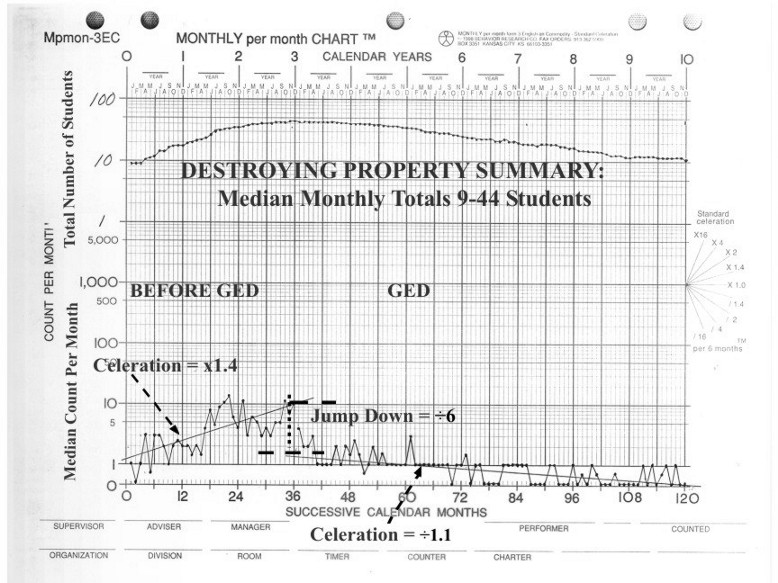
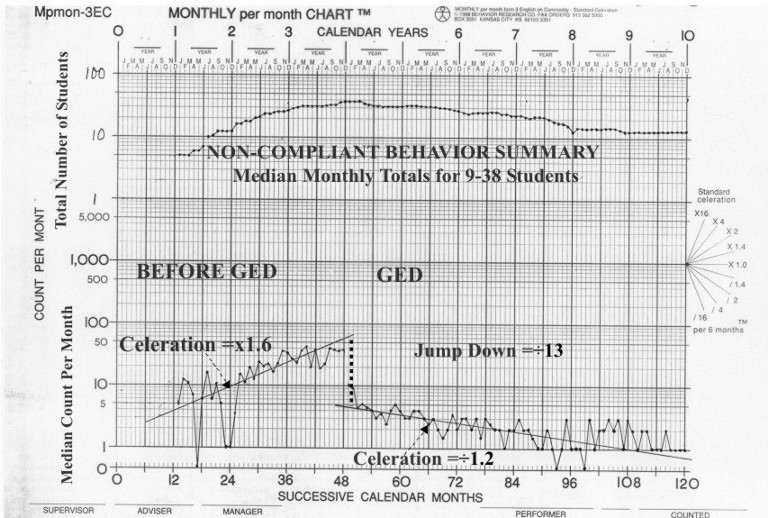
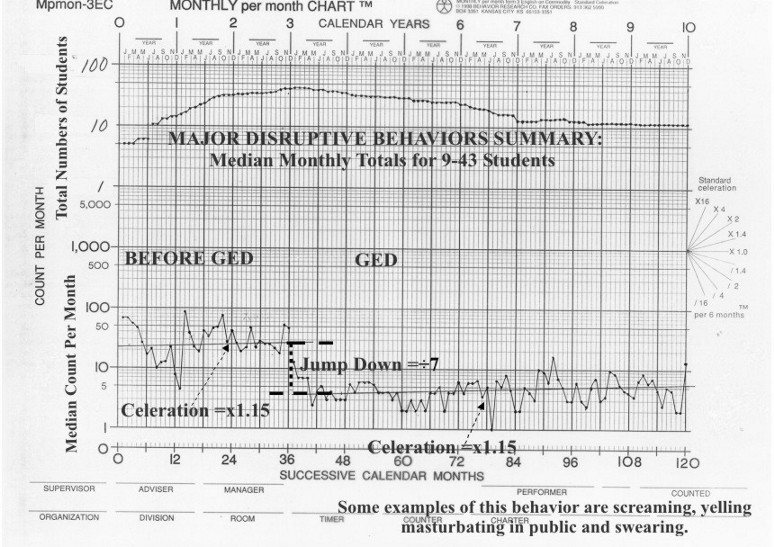
Exhibits 49-54 are Month Summary Charts for the five major behavior
categories we have treated. Each dot on these charts represents the
median of from 15 –63 students during the months before the start of use of
the GED/GED4 and during the months after the change to the GED/GED4. Because not
all students had the same length of time before or after the start of the GED/GED4
procedure, the dots on the chart do not all represent the same number of
students. The number students whose monthly totals are averaged in each dot is
shown in the chart at the top of the chart. During the months immediate before
and after the intervention, however, pretty much the same number of students are
averaged in each dot. For example, the dot for the month immediately preceding
the insertion of the GED and the dot for the month immediately after the GED/GED4
intervention are both medians of all 63 students.
This first chart (Exhibit
49) shows the median monthly totals, summarized across
all students, for health dangerous behavior (self-abuse, mainly). The chart
shows the typical result when GED was introduced. The frequency of the behavior
makes in immediate decrease ("jump-down") by a large factor (here by a
factor of 9) and then shows a deceleration after that point (here the frequency
decelerates by dividing by a factor of 1.1 every 6 months).
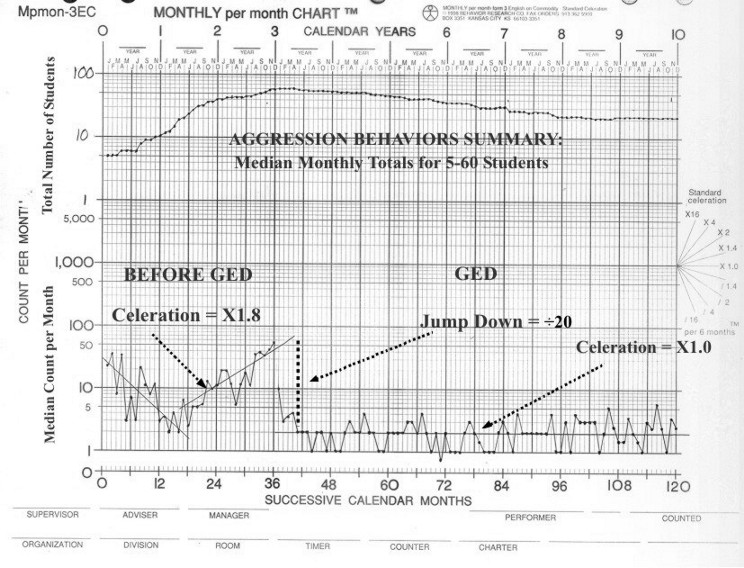
Similar results may be seen in the summary monthly charts for Aggression (Exhibit
50), Destroying Property (Exhibit
51), Noncompliance (Exhibit
52) and
Major Disruptive (Exhibit
53).
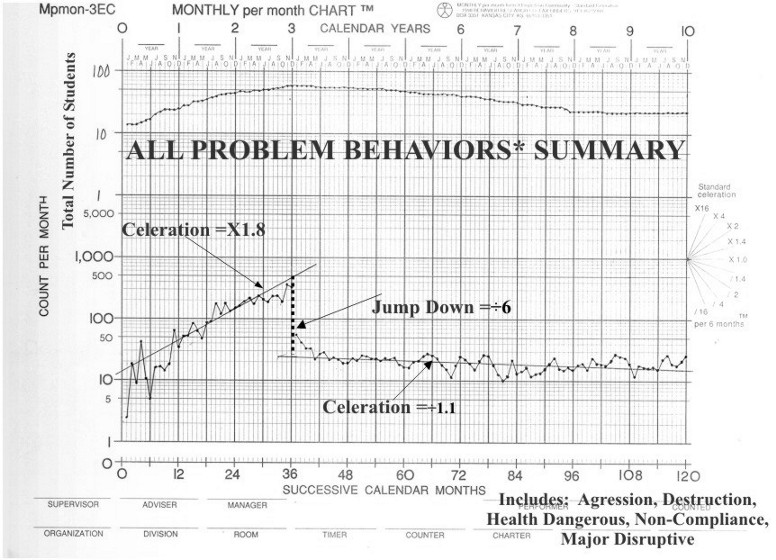
Exhibit 54 is a monthly chart that totals all five of the monthly charts you
have just seen. For each student we obtained the total of all of the 5 major
problem areas and then took the median for those totals. The resulting chart
shows the same typical result we have seen in the individual component charts.
Exhibit 55
takes the same data I showed in the last six monthly charts and
plots it on a yearly chart. In other words, here we obtain the yearly
total for each student’s problematic behaviors in the years before and after
the introduction of the GED. Then we take the median of all of those yearly
totals and plot it in one dot. The result is the same we have already seen— a
very significant immediate jumpdown in each case and a subsequent deceleration
in all cases except one.
This last yearly chart (the "All Combined") summarizes a huge amount
of data. Each dot just before and after the change to the GED averages
approximately 66 full years of data in that one data point!
Discoveries/conjectures, based on our experience with skin-shock.
Effective over long period (up to 10 years).
Desirability of treating earliest possible phase of the behavior
Treatment of a wide variety of behaviors is feasible.
Simultaneous treatment of all behaviors is feasible.
Potential for preventive use (behavioral rehearsal lessons)
Usefulness of negative reinforcement paradign
Start with the most intense stimulus available and safe (avoid working up
the intensity ladder)
Desirable features of device:
- Adequately high intensity level
- Wire-attached electrodes
- Spread electrodes
- Multiple electrodes
Effectiveness through verbal mediation
Holidays from treatment may promote recovery from adaptation.
Absence of side effects
Skin-shock, combined with rewards and education should be considered as a
treatment of first resort, in preference to
- Strongly sedating medications
- Protective devices (splints, helmets, gloves, restraints that must be worn
continuously)
- Exclusion from society
- Insufficiently effective "positive-only" procedures
For further information, see two web sites:
- JRC’s Web Site:
http://www.Judgerc.org
Web Site on Effective Treatment of Case-Hardened Behaviors http://www.geocities.com/effectivetreatment
Purpose: to promote communication and information about effective treatment
procedures, including use of skin shock
Content:
- Papers on use of the skin-shock that have not been published elsewhere,
such as this paper
- Bibliography of approximately 100 references on the use of Skin Shock in
behavioral treatment
Back to EMEAB4 Symposium
Back to Main page
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}