|
Use of Skin-Shock at the Judge Rotenberg Educational Center (JRC) |
Effectiveness of Intense Positive Programming and Supplemental Contingent Skin Shock Device in Reducing the Frequency of Severe Maladaptive Behaviors for Individuals in a Residential Treatment Center
Matthew L. Israel, Ed Langford, Robert E. von Heyn, Nicholas Lowther, Patricia Rivera, Heather Sutherland, Krystal Sowersby & Maryellen Kelley
Judge Rotenberg Educational Center
Introduction
The Judge Rotenberg Educational Center operates day and residential programs for children and adults with severe behavior disorders with a wide range of diagnoses that have included conduct disorder, psychosis, autism or developmental disabilities. The basic approach taken at JRC is the use of behavioral psychology and its various technological applications, such as behavioral education, programmed instruction, precision teaching, behavior modification, behavioral counseling, self-management of behavior and chart-sharing. The behavior modification treatment for some individuals included court approved use of the Graduated Electronic Decelerator (GED), a contingent skin shock device, to decelerate specific targeted behaviors after positive programming had proven insufficient. The present report describes the effectiveness of the GED with 36 individuals referred to the Judge Rotenberg Educational Center (JRC) for treatment of their intense aggression, self-injury and other disruptive behaviors.
Methods
Participants
Thirty six residential clients that attended the Judge Rotenberg Center participated in this study. This group represented all clients that had their behavioral treatment program supplemented with the GED between May 2003 and May 2005. They were referred from Massachusetts, New York, Virginia and Maryland. Ages ranged from 10 years old to 34 with an average age of 16.9 years. Of these clients 73% were verbal and 27% were considered nonverbal. The primary Diagnosis for 49% was Mental Retardation for 51% some other DSM-IV-R diagnosis.
Apparatus
The remote activated contingent skin shock used was the Graduated Electronic Decelerator (GED) developed by this program in 1990. The GED was register with the FDA as a medical device. The output was 15 mA RMS for a 2-second duration. A 24-hour a data recording sheet was used to identify each targeted behavior and the data were placed into a charting database daily. A digital video recording system was used across all settings and allowed for live or archived viewing.
Procedure
All participants were initially treated with highly structured behavior plans that used a variety of Differential Reinforcement of Other Behaviors (DRO) contracts. Contract lengths varied between 5 minutes and 7 days, depending on the frequency of the targeted behaviors. Reinforcers were individualized for each participant and based, when possible, on their verbal preferences. An economy, in the form of points or tokens, was also in place for each participant. Points/tokens were awarded for passing contracts, completing academics or exhibiting other defined prosocial behaviors. Points/tokens could be spent in a variety of ways to purchase preferred items or activities. A response cost system was also in place whereby points/tokens were deducted when targeted behaviors occurred. Prior to the use of GED, when participants exhibited aggressive or self-injurious behaviors, emergency physical or mechanical restraints were employed. Chemical restraint was never used. For more information on JRC’s programs visit www.judgerc.org.
For the 36 participants, as evidenced from the behavioral charts, the positive only approach did not produce a clinically significant improvement in their targeted behaviors. These behaviors interfered with their entire educational and habilitative programming and posed a significant risk of injury. Therefore, at various intervals after intake, JRC petitioned the Probate Court in Massachusetts for permission to use the Graduated Electronic Decelerator (GED) to treat their challenging behaviors. The proposed treatment plan presented to the Court, written by a doctoral level psychologist or clinician, operationally defined the behavior topographies to be treated with the GED. When GED treatment began, the individual’s daily recording sheet described those topographies for which the clinician prescribed GED treatment. To insure reliable treatment, two therapists confirmed the existence of the targeted behavior on the individual’s daily recording sheet before the GED consequence was administered. www.effectivetreatment.org.
Results
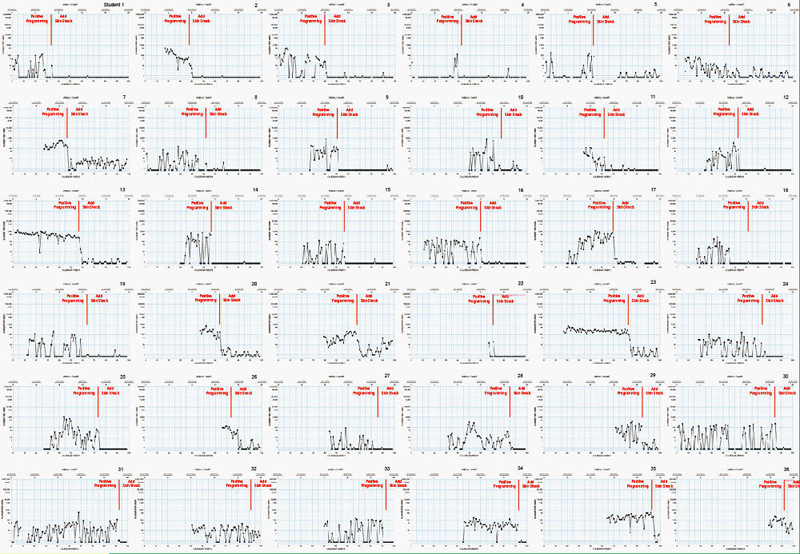
The attached Figures 1 through 3, depict weekly standard celeration charts for the most recent 36 students to begin GED treatment. Each figure shows 36 charts, corresponding to these 36 students. The charts are labeled 1 to 36, such that the chart labeled “Student 1” represents data for the same student across all 3 figures. The aim of this treatment was to reduce rates of aggressive, health dangerous and major disruptive behaviors. The data at the far right of the charts represents the last week of May, 2005. Charts vary in length, depending on the amount of time each student has spent at JRC, with the shortest chart (Student 36) displaying 21 weeks of data and the lengthiest chart (Student 1) displaying 100 weeks of data. Within each chart, the vertical dark line represents the initiation of GED treatment. For example, Student 1 (top left) began treatment in January of 2004, while Student 36 (bottom right) began treatment in March of 2005.As can be seen in most of the charts, the introduction of GED treatment reliably produces a rapid decrease in the response rates of targeted behaviors. This is true across all individuals and behaviors.
Prior to GED intervention, median rates[1] of aggressive responding ranged between 0 and 460 per week across the 36 students (Figure 1)1. Following intervention, weekly median rates ranged from 0 to 21. Before GED treatment, just 8% of students were maintaining a median rate of zero per week, but with high variability. Following the introduction of GED treatment, 72% of those same students maintained a weekly median of zero instances of aggression, and 94% of those students’ rates of aggressive responding were maintained at a weekly median of fewer than 5. Also worth noting is that response rates were not highly variable. That is, they were maintained at steady, low rates when treated with GED.
Figure 1 Aggression
Chart for 36 Students May 2003 - May 2005
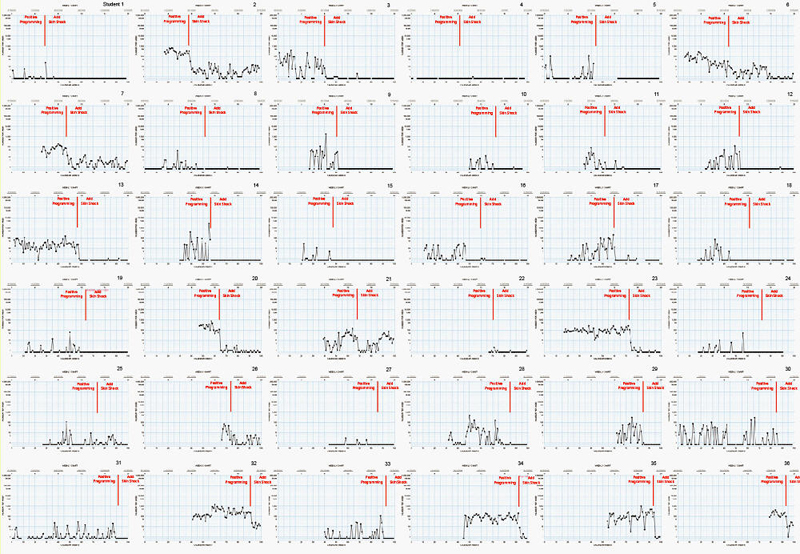
Health dangerous responding, depicted in Figure 2, reduced in similar fashion. Without GED treatment, weekly median rates of responding ranged from 0 to 240, whereas the range decreased to between 0 and 11 with GED treatment. The percentage of these students maintaining median rates of zero per week prior to GED treatment was 39%. This percentage jumped to 75% with GED treatment, while 94% had weekly medians of 5 or fewer. Again, when treated with GED, health dangerous responding did not occur at highly variable rates.
Figure 2 Health
Dangerous Chart for 36 Students May 2003 - May 2005
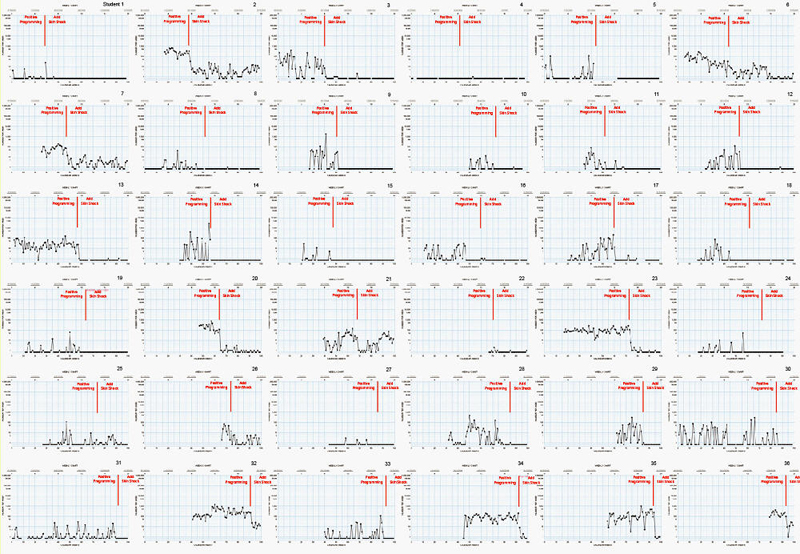
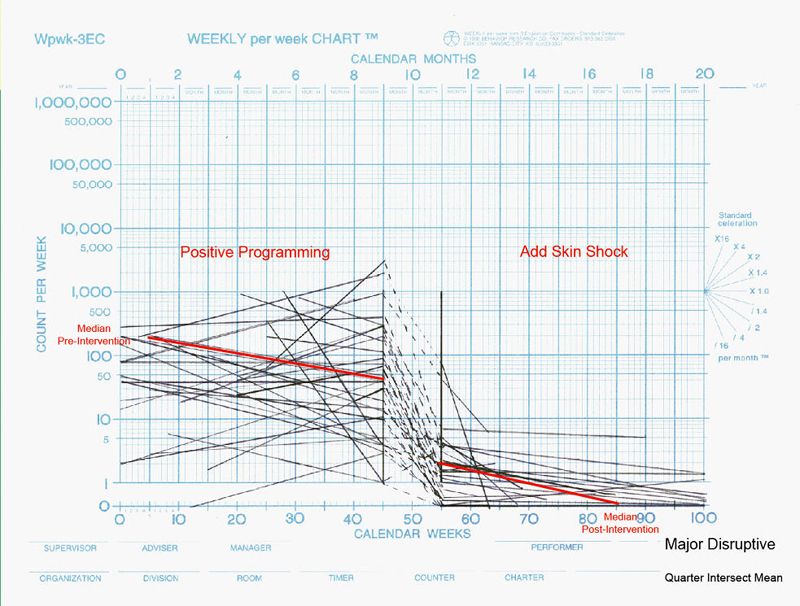
Major disruptive behavior, shown in Figure 3, was also dramatically reduced when treated with the GED. Prior to GED treatment the weekly median rates ranged from 0 to 1,224 and was highly variable. When treated with GED these median rates ranged from 0 to 15. With GED treatment, 34 of the 35 or 94% showed a reduced rate of responding such that weekly median rates were under 10. As with the other two categories of behavior, major disruptive behavior was maintained at low, steady rates with little variability.
Figure 3 Major
Disruptive Chart for 36 Students May 2003 - May 2005
Figures 4 to 6 show a celeration collection of all individuals included in this paper across the aggressive, health dangerous and major disruptive categories. The left hand portion of each chart depicts weekly celeration of the targeted behavior with positive only programming. The center portion of each chart depicts the jump down or up in response rate when GED was first introduced and the right hand portions depicts the celerations with GED treatment. It is clear in all three Figures that the introduction of the GED led to a substantial jump down in response rates in almost every case. Figure 4 shows that the GED treatment maintained near zero rates for 33 of the 36 individuals. Figure 5 shows that the health dangerous behaviors of 35 of 36 individuals maintained low or zero rates with GED treatment. Only one individual, who showed an initial jump down, had an accelerative trend. Figure 6 shows that the major disruptive behaviors of 33 of 35 individuals maintained low or zero rates with GED treatment. Two individuals, who showed an initial jump down, had an accelerative trend with GED treatment.
Figure 4
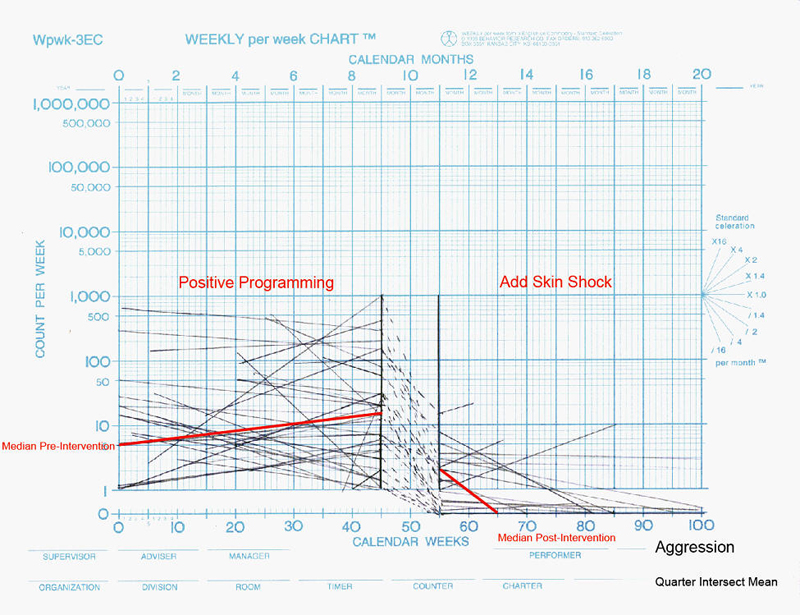
Figure 5
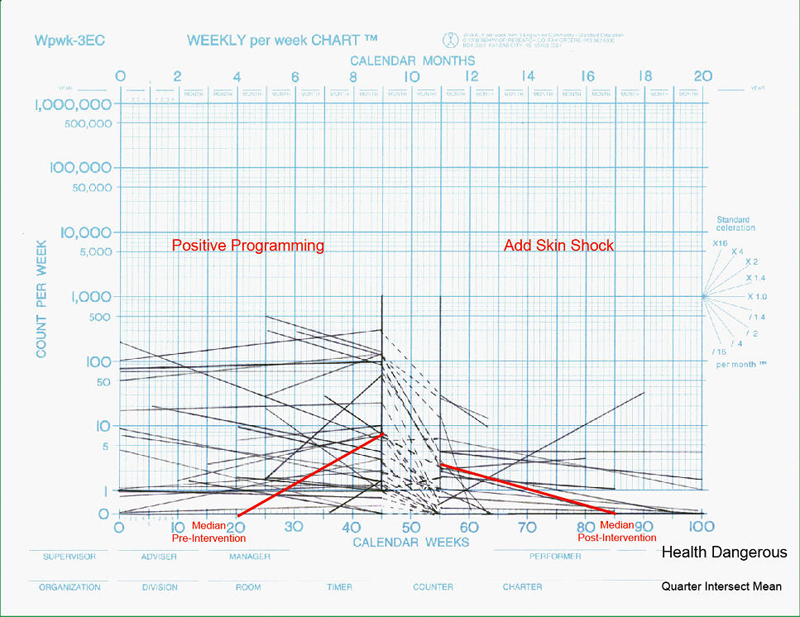
Figure 6
Discussion
JRCs behavioral program, rich in positive reinforcers, supplemented with a
punishment component to rapidly decelerate inappropriate behaviors, produced no
negative side effects and allowed medications to be eliminated. All 36
individuals required emergency physical or mechanical restraint prior to the
introduction of GED treatment but it is no longer necessary for any of them. In
many of the cases presented the GED was totally weaned from their program or is
in the process. Equally important it allowed these individuals to actively
engage in an educational curriculum, live in community-based apartments and, in
some cases, become gainfully employed. In many cases family contact was
reestablished and peer relationships improved. While this method may be
considered intrusive, many of the individuals and all of their families welcomed
this treatment and credited treatment success to it. The majority of individuals
admitted to JRC, approximately 60%, responded well to the positive-only
behavioral program. The other 40% however did not show a sufficient reduction in
the behaviors that led to their referral and admission to JRC. With further
research it may prove that this procedure is the most effective, least intrusive
treatment available for individuals such as these who have only worsened under a
myriad of medications, psychotherapy and weaker treatment programs.
[1] It needs to be noted that a weekly median of 0 does not indicate the absence of behavior, but that the individual had more weeks without any instances of aggression than weeks with instances of aggression.