
|
Use of Skin-Shock at the Judge Rotenberg Educational Center (JRC) |
Treatment of Severe Aggression and Self-Injury with Contingent Skin Shock with Individuals with Psychiatric Diagnoses without Developmental Delays
Robert E. von Heyn, Matthew L. Israel, Robert W. Worsham,
Maryellen Kelley, Susan Parker & Lynn Parrillo,
Judge Rotenberg Educational Center
Canton, MA USA
We examined the effectiveness of a behavioral treatment program for 8 individuals with various DSM-IV-TR psychiatric diagnoses who did not have developmental delays. The basic approach was the use of behavioral psychology and its various technological applications, such as behavioral education, programmed instruction, precision teaching, behavior modification, behavior therapy, behavioral counseling, self-management of behavior and chart-sharing. For these 8, the behavior modification treatment included court approved use of the Graduated Electronic Decelerator (GED), a contingent skin shock device, to decelerate specific targeted behaviors. All 8 cases studies presented had failed to improve with more typical treatments using psychotherapy, medications and less intrusive forms of behavior modification. With the supplement of the GED these individuals showed dramatic deceleration of targeted behaviors and dramatic acceleration of academic, vocational and pro-social behaviors. The results of the treatment programs were long-lasting with 4 of the cases successfully transitioned to less intrusive settings, including going back home, and the other 4 either partially or completely weaned off the GED. With further research it may prove that this procedure is the most effective, least intrusive treatment available for individuals such as these who have only worsened under a myriad of medications, psychotherapy and ineffective treatment programs.
The Judge Rotenberg Educational Center operates day and residential programs for children and adults with behavior problems, including conduct disorders, emotional problems, brain injury or psychosis, autism and developmental disabilities. The basic approach taken at JRC is the use of behavioral psychology and its various technological applications, such as behavioral education, programmed instruction, precision teaching, behavior modification, behavior therapy, behavioral counseling, self-management of behavior and chart-sharing. The behavior modification treatment included court approved use of the Graduated Electronic Decelerator (GED), a contingent skin shock device, to decelerate specific targeted behaviors for some individuals. The present report describes the effectiveness of the GED with eight individuals referred to the Judge Rotenberg Educational Center (JRC) for treatment of their intense aggression, self-injury and other disruptive behaviors such as property destruction and noncompliance. Case studies are presented detailing the rapid deceleration of targeted behaviors and the subsequent positive side effects following the treatment of these behaviors with individuals with various DSM-IV-R diagnoses, including Severe Depression, Bipolar Disorder and Schizophrenia without mental retardation. These individuals are not typical of those that have been treated with contingent electric shock as reported in the psychological literature. Most published articles have dealt with individuals with more severe cognitive impairments, developmental delays and/or autism. However, a common factor between these individuals and those described in the literature are their intense aggressive and self-injurious behaviors that had not responded to more traditional treatments. For these individuals, medications, positive-only behavior modification and traditional types of psychotherapy had failed to produce a significant impact on their interfering behaviors. In conjunction with the treatment to decelerate these inappropriate behaviors, academic education, daily living skills, social skills and community integration were taught. Information on previous treatments, number of placements, diagnoses and grade level are presented. Frequency data of targeted behaviors were collected hourly and plotted on daily, weekly and monthly charts. Other areas of improvement in these individuals’ living and working environments and development of new skills are also provided.
Method
All participants were initially treated with highly structured behavior plans that used a variety of Differential Reinforcement of Other Behaviors (DRO) contracts. Contract lengths varied between 5 minutes and 24 hours, depending on the frequency of the targeted behaviors. Reinforcers were individualized for each participant and based on their verbal preferences. A token economy, in the form of points, was also in place for each participant. Points were awarded for passing contracts, completing academics or exhibiting other defined prosocial behaviors. Points could be spent in a variety of ways to purchase preferred items or activities. A response cost system was also in place whereby tokens were deducted when targeted behaviors occurred. When participants exhibited aggressive or self-injurious behaviors, emergency physical or mechanical restraints were employed. Chemical restraint was never used. For more information on JRC’s programs visit www.judgerc.org.
For these participants, the positive only approach did not produce a clinically significant improvement in their targeted behaviors. These behaviors interfered with their entire educational and habilitative programming and posed a significant risk of injury. Therefore, at various intervals after intake, JRC petitioned the Probate Court in Massachusetts for permission to use the Graduated Electronic Decelerator (GED) to treat their challenging behaviors. The GED is an FDA registered medical device that administers a 2-second skin shock when remotely activated by a therapist. The proposed treatment plan presented to the Court, written by a doctoral level psychologist or clinician, operationally defined the behavior topographies JRC requested for treatment with the GED. When GED treatment began, the individual’s daily recording sheet described those topographies for which the clinician prescribed GED treatment. To insure reliable treatment, two therapists confirmed the existence of the targeted behavior on the individual’s daily recording sheet before the GED consequence was administered. Twenty-four hour a day videotaping and live monitoring also insured treatment consistency. For more information on the GED see www.effectivetreatment.org.
ES—Figure 1
· Beginning at the age of three, 2 residential and day school programs, 2 psychiatric hospitalizations, and home instruction prior to admission to JRC. Discharged from all but one placement due to the severity of her aggressive and health dangerous behaviors, repeated elopement, suicidal ideation and continued defiance.
· Past treatments included psychotherapy, group and individual therapy.
· Medications included Ritalin, Dexedrine, Risperdal, and Depakote.
· Diagnoses: Atypical Psychosis, ADHD; Conduct Disorder, childhood onset type; Oppositional Defiant Disorder and Major Mood Disorder.
· Targeted behaviors included physical aggression and self-injurious behaviors that encompassed assaulting her sister, hitting her teacher with a baseball bat, biting others, cutting herself with sharp objects, running away, and ingesting household cleaners.
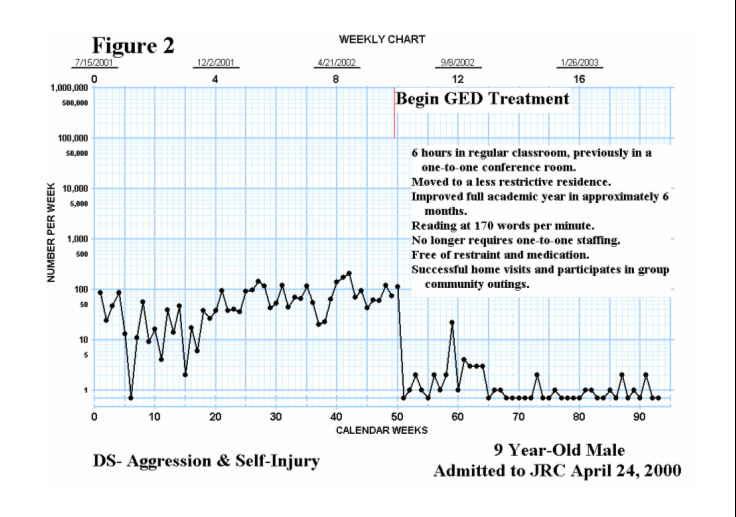
DS—Figure 2
· Beginning at the age of two and a half, 2 day school programs and 3 psychiatric hospitalizations, including for 6 months prior to admittance.
· Past treatments included group and individual therapy.
· Medications included Cylert, Clonidine, Adderal, Risperdal, and Haldol.
· Diagnoses: Psychosis, NOS, and ADHD.
· Targeted behaviors included physical aggression and self-injurious behaviors that encompassed striking another child with a seatbelt buckle on the school bus, killing his kitten, attempted to stab a child with a pencil, sexual acting out, tying belts around his neck, assaulting his mother and siblings, and running into the street and traffic.
· Physical and mechanical restraint required frequently at JRC.
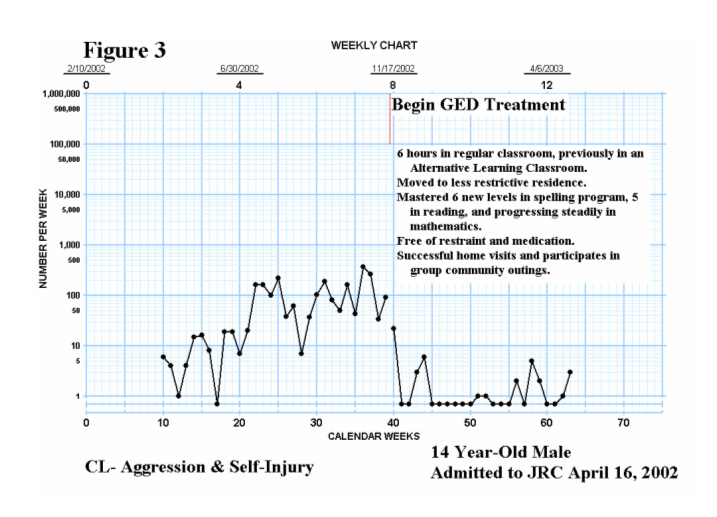
CL—Figure 3
· Beginning at the age of seven months, placed in 1 foster home, 1 day school program, 1 residential school and treatment program, 4 short-term psychiatric hospitalizations, and 1 long-term psychiatric hospitalization. Discharged and readmitted to many of these placements due to uncontrollable aggressive and self-injurious behaviors.
· Past treatments included a behavior modification program that included earning daily rewards for “being safe”, physical restraints, group and individual counseling.
· Medications included Risperdal, Depakote, Cogentin, Ritalin, Zoloft, Lithium, Clonidine, Inderal, Mellaril, Olanzapine, Eskalith, Pamelor, Clozaril, Seroquel, and Paxil.
· Diagnoses: ADHD; and Mood Disorder, NOS.
· Targeted behaviors included aggressive and self-injurious behaviors that encompassed hitting himself and others with great force, head butting others, attempting to choke himself, head banging, and pounding on doors.
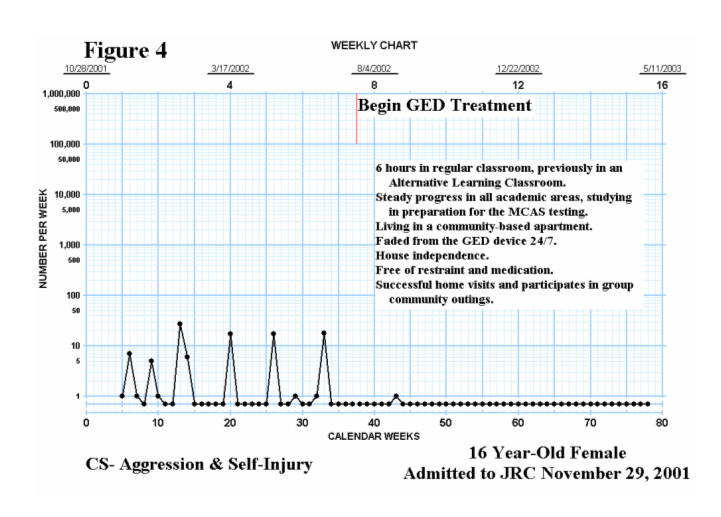
CS—Figure 4
· Previously in 2 residential and day school programs, 2 residential treatment facilities, and 4 psychiatric hospitalizations. Discharged from all of these placements due to uncontrollable aggressive and self-injurious behaviors.
· Past treatments included psychotherapy, group and individual therapy, physical restraints, milieu treatment, and less restrictive behavioral intervention programming.
· Medications included Depakote, Seroquel, Topomax, Risperdal, Ritalin, Paroxetine, and Celexa.
· Diagnoses: Mood Disorder, NOS; and Conduct Disorder.
· Targeted behaviors included aggressive and self-injurious behaviors that encompassed biting her mother, threatening family with knives multiple times, attempting to jump out a window, running away, cutting herself with sharps objects, suicide attempts, banging her head with the stated intent to dislodge her shunt, and attempting to overdose on medications.
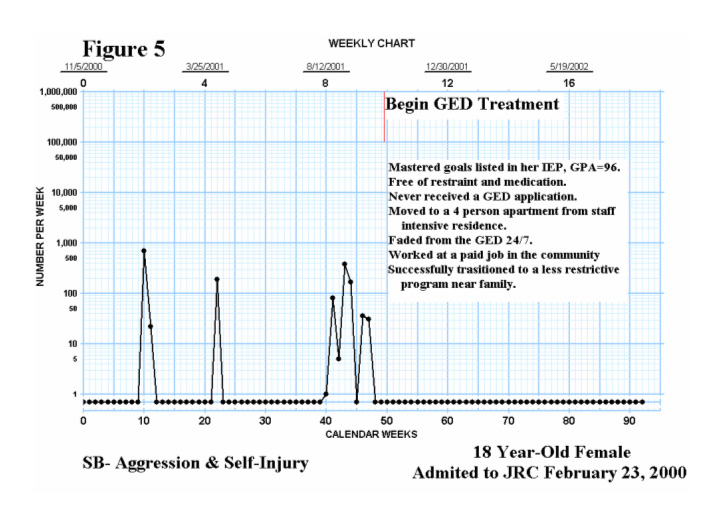
SB—Figure 5
· Beginning at the age of five, placed in 12 different foster homes, one residential placement, one detention center on two occasions, and one psychiatric hospitalization. Discharged from all of these placements due to uncontrollable and frequent aggressive and self-injurious behaviors.
· Past treatments included counseling and psychotherapy.
· Medications included Zoloft, Lithium, and Tegretol.
· Diagnosis: Bipolar Mood Disorder.
· Targeted behaviors included aggressive and self-injurious behaviors that encompassed pushing a parent down a flight of stairs, throwing a television and chairs at staff members, running away, ingesting large amounts of alcohol, suicidal ideation, and cutting herself with objects.
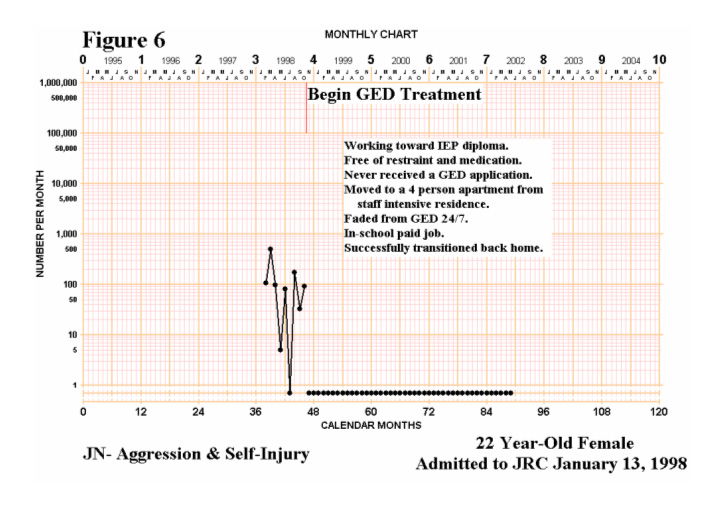
JN—Figure 6
· Beginning at age 11, required six psychiatric hospitalizations. Discharged and readmitted to many of these due to uncontrollable aggressive and self-injurious behaviors.
· Past treatments included counseling, four-point restraint, and emergency medication.
· Medications included Mellaril, Depakote, Lorazepam, and Prolixin.
· Diagnoses: Intermittent Explosive Disorder and Conduct Disorder Childhood Onset Type.
· Targeted behaviors included aggressive and self-injurious behaviors that encompassed stabbing her sister with a knife, threatening her mother and sister
· Targeted behaviors included aggressive and self-injurious behaviors that encompassed stabbing her sister with a knife, threatening her mother and sister on several occasions with knives, cutting a principal’s hand with a box cutter she brought to school, holding a knife and threatening to kill herself, and banging her head.
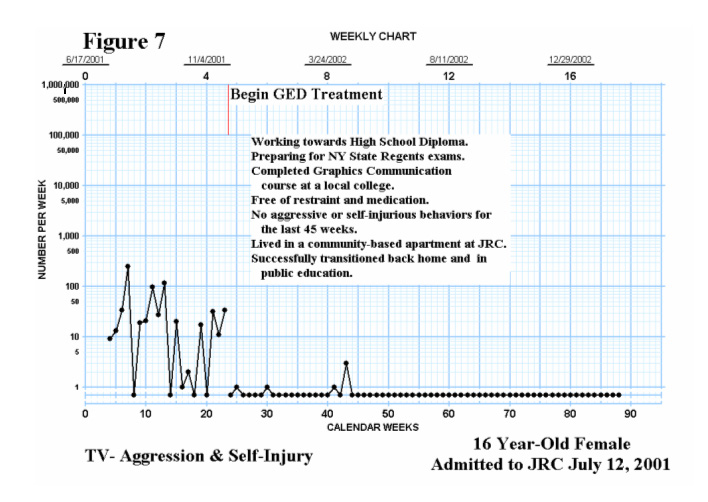
TV—Figure 7
· Previously in three residential placements and rejected from six residential treatment programs prior to JRC due to severe aggressive and self-injurious behavior.
· Past treatments included psychotherapy and frequent restraints (physical, mechanical, and chemical).
· Medications included Seroquel and Depakote.
· Diagnoses: Bipolar Disorder NOS, Conduct Disorder – Child Onset.
· Targeted behaviors included aggressive and self-injurious behaviors that encompassed hitting her mother and threatening her grandmother, fist fights with males and females, pulling others hair, and running away.
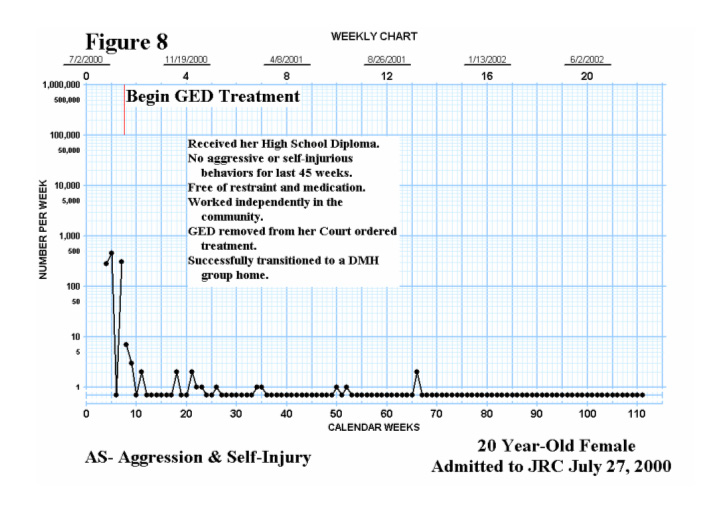
AS—Figure 8
· Previously in 2 foster homes, 4 residential placements, 4 psychiatric hospitalizations and 1 emergency respite program. Discharged from each due to continued aggression and self-injury and inability to keep her and others safe.
Medications included: Klonopin, Lithium, Wellbutrin, Seroquel, Tegretol, Cogentin, Prozac, Ritalin,
· Thorazine, Naltrexone, Depakote, Clonidine, Zyprexa, Trilafon and Haldol.
· Past treatments included ‘intensive behavioral programming’, milieu therapy and group and individual therapy and physical and mechanical restraint.
· Diagnoses: Post Traumatic Stress Disorder and Mental Disorder, NOS due to lead poisoning.
· Targeted behaviors included physical aggression and self-injurious behaviors including head banging, runaway, tying material around her neck, scratching open her skin with objects or fingernails and imbedding staples and paperclips under her skin.
Results and Discussion
Figures 1 through 8 contain the behavior charts of the combined frequencies of aggressive and self-injurious behaviors and some of the positive effects of GED treatment. Figures 1 through 4 depict data up to the present and Figures 5 through 8 show data up until the date of discharge from JRC. The data clearly indicate the efficacy of the behavioral treatment package in rapidly decelerating the rate of the targeted behaviors and the continued reduction to zero rates. The behavioral program, rich in positive reinforcers, together with a punishment component to rapidly decelerate inappropriate behaviors, produced no negative side effects and allowed medication and all restraint to be eliminated. Equally important it allowed these individuals to actively engage in an educational curriculum, live in community-based apartments and, in some cases, become gainfully employed. In all of these cases they jumped two or more academic grade levels in less than a year. In many cases family contact was reestablished, and peer relationships improved. While this method may be considered intrusive, the individuals and their families welcomed this treatment and credit treatment success to it. With further research it may prove that this procedure is the most effective, least intrusive treatment available for individuals such as these who have only worsened under a myriad of medications, psychotherapy and weaker treatment programs.
Table 1
The Effect of GED on Aggressive and Self-Injurious Behaviors
|
Participants |
Total 20 weeks Pre-GED |
Total for Last 20 weeks |
Total GED Applications |
Weeks of GED Treatment |
Median GED/week |
Immediate Effect of GED |
|
ES |
564 |
6 |
14 |
52 |
0 |
¸8 |
|
DS |
1,654 |
9 |
58 |
44 |
1 |
¸50 |
|
CL |
2,203 |
0 |
24 |
23 |
0 |
¸100 |
|
CS |
54 |
20 |
1 |
40 |
0 |
¸0 |
|
SB** |
703 |
0 |
0 |
44 |
0 |
¸20 |
|
JN** |
381 |
0 |
0 |
44 |
0 |
¸25 |
|
TV** |
703 |
0 |
6 |
65 |
0 |
¸6 |
|
AS** |
1,035* |
0 |
6 |
104 |
0 |
¸45 |
*only 3 weeks of data prior
to GED implementation
** discharged to less restrictive setting